| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
Tubercular Syphiloderm (Synonyms: Syphiloderma tubercu-
losum; Nodular syphiloderm or syphilid; Syphilis cutanea tuberculosa).—
The tubercular syphiloderm may exceptionally occur within the first year
as a more or less generalized eruption, of characteristic brownish-red or
ham-colored, small to large pea-sized tubercles, but even in such gen
eralized cases the lesions are usually, for the most part, more of the na
ture of papulotubercles (papulotubercular syphiloderm) than tubercles.
Less rare is it, although not at all common, to find papulotubercular and
tubercular lesions on the face, especially about the nose, forehead, and
chin, and somewhat crowded together, in association with the typical
papular eruption on other parts. As a rule, however, it is a tertiary mani-

Fig. 192.—Tubercular syphiloderm, with slight ulcerative tendency; showing the char
acteristic spreading border; of several years’ duration.
festation, appearing several or more, sometimes many, years after the
contraction of the disease; limited in extent and appearing on one or sev
eral regions, and exhibiting a decided tendency to occur in groups of
segmental, circinate, and serpiginous configuration.
The tubercles are of the same characters in the late, limited mani
festation as in the rare generalized cases. They present commonly as
several or more groups of somewhat firm, circumscribed, slightly or mod
erately elevated lesions extending into the corium and sometimes more
deeply. They have a smooth surface, with often a glistening aspect,
or covered with thin epidermic exfoliating scales; are rounded or acu
minated in shape, occasionally somewhat flattened and of a brownish-
red or coppery color, and usually the size of small or moderately sized
peas. They are, as a rule, closely set together, forming a segmental
or ring-like grouping, and showing often a tendency to actual and intimate
8o4
NEW GROWTHS
coalescence. Several contiguous groups may coalesce and form a ser-
piginous tract of an irregular, winding, snake-like character; or the older
lesions of a segmental or circinate group disappear, new ones appearing
on the outer edge or just beyond the border, and in this manner the seg
ment or circle enlarges, in a slowly creeping manner, the lesions within
this spreading border undergoing involution, and leaving a pigmented,
often atrophic, area behind, constituting the so-called serpiginous tuber
cular syphiloderm. Where the creeping and widely extending tendency

Fig. 193.—Tubercular syphiloderm with ulcerative tendency, and showing the well-
defined spreading border; of one to two years’ duration.
is not exhibited, the terms circinate tubercular syphiloderm and seg-
mental tubercular syphiloderm are sometimes employed, according to
circumstances. The individual lesions usually develop slowly, are
sluggish in their course, remaining at times for weeks or months without
material change. As a rule, however, they terminate sooner or later in
absorption and exfoliation, leaving, as already described, a more or less
permanent pigmentation, with or without slight atrophy or cicatricial
thinning, the disease continuing by the formation of new lesions appear
ing at the edge or closely adjacent. This form of the eruption, in which
SYPHILIS 805
ulcerative tendency is not displayed, is not at all uncommon, and is
known as the non-ulcerating tubercular syphiloderm, with often the
additional qualifying terms, circinate, segmental, or serpiginous, accord
ing to the configuration. In a few of these cases the scaliness may be
more pronounced than ordinarily observed, and have a psoriatic appear
ance, and such examples are sometimes termed tuberculosquamous
syphiloderm or squamous syphiloderm. In other instances, especially
when about the nose, the lesions may partake of the nature of both
papules and tubercles,—papulotubercles (papulotubercular syphiloderm),
—and some of which sometimes break down centrally and form pus
tules (tuberculopustular syphiloderm) which may leave pit-like scars.
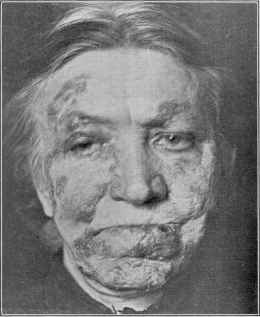
Fig. 194.—Tubercular syphiloderm, with but little destructive tendency, showing the
segmental configuration; of several years’ duration.
In the majority of cases, however, of the tubercular syphiloderm,
instead of the lesions undergoing absorption and exfoliation, ulcera-
tion takes place, and this may be displayed from the beginning or occur
after a well-formed group or patch has lasted for some weeks, consti
tuting the ulcerating tubercular syphiloderm. The patches or groups
have the same tendency to the special configurations of segmental,
circinate, and serpiginous, already mentioned, and hence one of the de
scriptive terms, depending upon the characters displayed, is sometimes
added, giving rise to the names “ulcerating serpiginous tubercular syphil-
oderm,” etc In these cases there are, therefore, found tubercles, ulcera-
tions, and usually crusting. The ulceration may be superficial or deep
in character, and involve several or all the lesions forming the group.
This may consist, therefore, of small, discrete, punched-out ulcers, or
8o6
NEW GROWTHS
one or more continuous ulcers of segmental, crescentic, or serpiginous
shape. Ordinarily they are quite shallow, although in some cases the
ulceration extends to considerable depth. They are either covered with
a gummy, grayish-yellow, purulent secretion, or are crusted, the secre
tion drying to crusts. Not infrequently the patch spreading peripher
ally shows an extending, elevated, infiltrated border, made up of closely
contiguous or coalescent tubercles, which have lost their individuality
and form a line of infiltration, which, toward their inner border, have
already undergone ulceration, usually covered with crusts; and so the
patch gradually invades the surrounding healthy surface, while, as a
rule, healing with consequent cicatricial tissue, and commonly more
or less yellowish-brown or brownish pigmentation, are noted on the part
already traversed. In some instances the tubercles form into closely

Fig. 195.—Tubercular syphilodcrm with ulcerative tendency, of a year’s duration,
showing the clearing central portion and spreading border.
packed areas of infiltration, the patch presenting both tubercular and
gummatous characters, often rapidly ulcerating in places or more or
less uniformly; or the lesions, while close but discrete, may also occa
sionally be of a mixed tuberculogummatous nature; such cases give rise
to the term tuberculogummatous syphiloderm.
Sometimes there is but a sluggish tendency toward healing, and
the ulcerations show a disposition to papillary hypertrophy or vegeta
tions, with an offensive, yellowish or greenish-yellow, puriform discharge,
probably occurring most frequently upon the scalp, constituting, again,
as referred to in some cases of moist papules, the modification or variety
often designated the papillomatous or vegetating syphiloderm or syphilid
(also called syphilis cutanea papillomatosa, syphilis cutanea vegetans).
Exceptionally the ulcerated segmental groups crust over, gradually ex-
SYPHILIS
807
tend, and become crusted over with several or more stratified layers of
crust, the smallest at the top, oyster-shell like, as observed in the rupial
formation of the large flat pustular syphiloderm. The favorite region
is the face, especially the region of the nose and mouth, but it is quite
common also on the upper part of the trunk, and the arms and legs;
in fact, no region is exempt. It may be, and commonly is, limited to
one region, but not infrequently areas of small or large size are seen on

Fig. 196.—Tubercular syphiloderm involving arm and forearm, of several years’
duration, showing the serpiginous spread and the small soft scars of the earlier eruption;
disease contracted some years previously.
two or more parts. There are generally no subjective symptoms,
although occasionally the ulcerations are tender and painful. Its
course is usually slow, and while there is, as a rule, a tendency displayed
toward involution or ulceration and healing in the older lesions, new
tubercles continue to appear, so that complete spontaneous cure, while
it may occasionally result, is not to be expected, and the eruption con
tinues indefinitely. It is, however, almost invariably rapidly responsive
to specific constitutional treatment.
8o8
NEW GROWTHS
The diagnosis of the tubercular syphiloderm is, as a rule, not diffi
cult, although it often resembles closely lupus vulgaris. The differ
ential points are considered under this latter disease. The diagnostic
features of this syphiloderm are the tendency to form segments, crescents,
or circles, its method of spread, the color, ulceration, pigmentation, and
atrophy or scarring of the older part; these, together with the history,
and sometimes marks or scars of former syphilitic eruptions, are usually
sufficient to warrant a conclusion.

Fig. 197.—Tubercular syphiloderm with ulcerative tendency, of several years’
duration, showing segmental configuration and scars of earlier areas.
Confusion with epithelioma, acne rosacea, leprosy, sycosis, psoriasis,
and ringworm has occurred, but such errors are almost invariably the
result of hasty examination or inexperience, as the several diagnostic
features of the tubercular syphiloderm, when considered together,
furnish sufficient grounds of difference, without mentioning the differen
tiating characters of the other diseases named. The lesion of epithelioma
is usually single, has an infiltrated, often roll-like border, and often the
peculiar, semitranslucent, pearly-looking tubercles or nodules adjacent
or surrounding; it is generally much slower in its progress, the discharge
is not commonly profuse or offensively purulent, and is often mixed with
a little blood; it is more common after fifty, and somewhat infrequent
SYPHILIS
809
before this age—just the reverse of the tubercular syphiloderm. In
acne rosacea there is no segmental or circinate configuration, no distinct
ulcerations, the tubercles or nodules are, as a rule, vividly red, and dilated
capillaries are usually present.
When the tubercles or papulotubercles of syphilis are numerous
and crowded together on the face, a somewhat leonine aspect is given to
the countenance, and a suggestion of tubercular leprosy; but in cases
of the latter disease there are found symptoms such as a history of febrile
attacks, anesthetic patches, neuralgic and other nervous disorders, and
brown, pigmented areas. Sycosis vulgaris is follicular in origin, with
no tendency to ring-like or segmental configuration, and is not destruct
ive; that form known as ulerythema sycosiforme may, however, resemble
syphilis somewhat, but its follicular origin, slow progress, and usually
rather tough cicatricial formation, resulting not from distinct ulceration,
but atrophic changes, will serve to distinguish it. In ringworm sycosis,
if of the superficial type, there is the ring-like border, but this is not dis
tinctly infiltrated, and is lacking the ulceration and pea-sized brownish
tubercles found in syphilis. In the deep-seated ringworm sycosis the
subcutaneous nodulations or lumpiness are characteristic, especially
when taken together with the history of a follicular or ringworm patch
origin. The circinate tubercular syphiloderm has been mistaken
for ringworm of the non-hairy surface, but the absence of defined tuber
cles or infiltrated border, pigmentation and atrophy or ulceration and
scarring in the latter should serve to prevent mistake. The history is,
moreover, wholly different. In cases seemingly like ringworm, micro
scopic examination for the fungus would decide if doubt still remained.
The tuberculosquamous type of this syphilid does at times roughly sug
gest psoriasis ,but could scarcely be mistaken for it (see under Psoriasis
for differential points).
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |