| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
SARCOMA CUTIS
Synonyms.—Sarcoma of the skin; Sarcomatosis cutis; Fr., Sarcome cutané; Sar
comatose cutanée.
The cases may be conveniently, but somewhat arbitrarily, divided
into three classes: (1) Non-pigmented sarcoma, local or generalized; (2)
melanotic sarcoma; (3) multiple pigmented (hemorrhagic) sarcoma,
the last being that form originally described by Kaposi. This division
corresponds essentially to that adopted by De Amicis, whose observation
of sarcomatous cases has been unusually extensive.1
Primary Single or Localized Non-pigmented Sarcoma.—This is a
relatively less malignant type of sarcoma than other forms, and may
remain as a single or localized, slowly growing tumor for some months
or years before destructive changes set in or more or less generalized
and metastatic growths appear. It varies considerably in size in dif-
1 De Amicis, Trans. Twelfth Internal. Med. Cong., at Moscow, 1897; abs. in Brit.
Jour. Derm., 1897, p. 440.
Some other valuable general literature: Perrin, “De la sarcomatose cutanée,”
These de Paris, 1886, with review of the subject and bibliography to date; Funk, “Klin-
ische Studien über Sarkome der Haut,” Monatshefte, 1889, pp. 19 and 60 (with numer
ous references); De Amicis, ibid., 1897, vol. xxv, p. 309 (with some references); Fordyce
gives a good account in Morrow’s System, vol. iii (“Dermatology”); J. C. Johnston (“Sar
coma and the Sarcoid Growths of the Skin”), Jour. Cutan. Dis., 1901, p. 305, reviews
the whole subject, illustrated by many admirable photomicrographs; Lieberthal, Jour.
Amer. Med. Assoc, Dec 6,1902, p. 1454 (with references); Pernet, “Congenital Sarco
mata,” Trans. Path. Soc’y, London, 1902, vol. liii, p. 360; Mallory, “Pathology of
Malignant Diseases of Non-Epithelial Formation,” Jour. Amer. Med. Assoc., No. 2,
1910, p. 1621.
894 NEW GROWTHS
ferent cases: it may be small, scarcely larger than a good-sized pea,
or more commonly the dimension of an egg or an orange. According
to Perrin, the original tumor rarely, if ever, exceeds the latter size.
In color it may remain almost that of the normal skin, but is usually
pale red or bluish, with often the surface showing dilated capillaries.
In some instances the blood-vessels of the tumor, which are generally
abundant, may be large and well developed—sufficiently so to give to the
touch a perceptible pulsation. In shape it may be nodular, encapsulated,
mushroom-like, or somewhat diffused in outline, and occasionally pedun-
culated. In its earliest stage it may be cutaneous or subcutaneous in
situation. It originates commonly from some local injury or other forma
tion, such as warts, vascular or pigmented nævi, sebaceous cyst, etc.,
or in some instances apparently from the healthy skin. It is met with
at all ages and in both sexes.
Generalized Non-pigmented Sarcoma.—In this form several or more
tumors may appear simultaneously at near or remote points, or it may
result from a primary single sarcoma, as already described, or in associa
tion with leukemia and pseudoleukemia. Arning, Joseph, Touton,
Wagner, Funk, and others (quoted by Fordyce) have reported, in con
nection with the latter affection, the general development of pea- to
walnut-sized, waxy, dark-red or bluish, cutaneous and subcutaneous
tumors, forming adhesions to the skin, with more or less intense itching,
and in some instances tending to break down and ulcerate. It is not
improbable that some of the cases associated with leukemia reported by
Biesiadecki, Kaposi (lymphodermia perniciosa), Hochsinger and Schiff,
Besnier, Vidal, and others have been more closely allied to granuloma
fungoides than to leukæmia cutis or to true sarcomatosis. Both Vidal
and Paltauf1 have called attention to this point. Some cases, too, of
generalized cutaneous distribution doubtless are secondary to an over
looked sarcoma in a visceral organ, in lymph-glands, testicle (Köbner),
parotid gland (Holden and Butlin). There are instances, however, in
which this type of generalized sarcoma seems primary in the skin. In
general non-pigmented sarcomata the skin overlying the tumors may be
close to the normal hue, with a reddish or bluish cast, or it may be,
especially later in the disease, of a dark-blue color. The growths, which
are somewhat variable as to size, as in primary single sarcoma, are
seated primarily either in the cutaneous or subcutaneous tissue, and may
be present in scanty numbers or extremely numerous, as in Cheever’s
case,2 a woman aged sixty-five, in whom all parts except the head were
the seat of nodular, ulcerating lesions, some of which underwent involu
tion. In other instances the growths are more or less crowded and lim
ited to one region, a rather remarkable example of which came under
the notice of Cohn,3 in which, in a woman aged fifty-two, the entire scalp
and temporal regions were the seat of numerous and bunched, cherry-
to egg-sized and larger growths.
1 Paltauf, “The Lymphatic Affections of the Skin,” Trans. Second Internat. Derm.
Cong., Vienna, 1889.
2 Cheever, Boston Med. and Surg. Jour., Jan. 14, 1885 (also seen by Dr. J. C.
White).
3 Cohn, Jour. Cutan. Dis., 1892, p. 393 (with illustrations).
SARCOMA CUTIS 895
This class of sarcomata, in some of its cases, approaches somewhat
closely to the third division—the multiple pigmented sarcoma of Kaposi;
and in others, especially the cases in which a tendency to ulceration is
exhibited, the similarity to granuloma fungoides is also striking, this
latter being considered by some observers as in reality a variety of sar
coma, a view that clinically, as to the tumor stage, has much apparent
support, but which is not borne out by the history, course of the malady,
and the histologic findings. Their occasional striking resemblance to
granuloma fungoides is recognized in the name proposed by Perrin for
this variety of this class,—generalized primitive pseudomycosic sarcoma-
tosis of the skin,—and also that by Funk, of multiple idiopathic gumma-
toid sarcomata of the skin, a suggestive example of which is reported by
Bowen,1 and another by Minne,2 and indicative of possible transition
cases. The course of generalized sarcomata is a variable one, and,
according to Perrin, death usually ensues within two years after the cuta
neous growths have appeared. The multiplication of the growths is
supposed to be due to dissemination of the morbific cells through the
agency of the blood circulation.
Melanotic Sarcoma.—This variety, the second class of De Amicis,
is the most malignant, usually running a rapid course. It is often con
fused with sarcomata of other varieties showing discoloration, but
between such and true melanotic sarcoma, as Hartzell3 states, a distinc
tion must be made; the coloring-matter of the latter is presumably a
product of the cells of the neoplasm, which frequently has its origin in
tissues normally pigmented, as the choroid and pigmented nævi, whereas
in the former the origin of the pigment is, for the most part, hematic.
If the conclusions of Unna,4 Gilchrist,5 Waelsch,6 Whitfield,7 Darier,8
and a few others9 are to be accepted,—that the cells in pigmented moles
which give rise to melanotic growths are in reality of epithelial origin,—
then the tumor of this variety thus originating must of necessity, as
these observers contend, be taken from the sarcomatous class and trans
ferred to the carcinomatous. In a recent valuable paper, Johnston10
1 Bowen, “Mycosis Fungoides and Sarcomatosis,” Jour. Cutan. Dis., 1897, p. 65.
2 Minne, Annales, 1899, p. 751.
3 Hartzell, “Sarcoma Cutis,” Jour. Cutan. Dis., 1893, p. 21.
4 Unna, Histopathology.
5 Gilchrist (“A Case of Melanotic Sarcoma, Primary in the Skin, in a Negro, with
Pathology”), Trans. Amer. Derm. Assoc. for 1898.
6 Waelsch, Archiv, 1900, vol. xlix, p. 249 (with 6 colored histologic cuts).
7 Whitfield, Brit. Jour. Derm., 1900, p. 267.
8 Darier, La Pratique Dermatologie, 1903, vol. iii.
9 Schalek (“Histogenesis of Melanosarcoma Cutis”), Jour. Cutan. Dis., 1900, p. 147,
has contributed a valuable, original, and review paper on this subject, based upon exami
nation of several cases. See also paper by Heitzmann (“Microscopic Studies on Mela-
notic Tumors of the Skin’’), Jour. Cutan. Dis., 1888, p. 201 (with illustrations), which
also has some bearing upon this point.
10 James C. Johnston, “Melanoma,” Jour. Cutan. Dis., Jan. and Feb., 1905. A
monograph that reviews the whole subject, with case citations, original investigations,
numerous histologic cuts, and complete bibliography. His conclusions are: 1. Aside
from the natural division into choroid and skin tumors, melanotic neoplasms, which,
from their diversity of origin, are best called melanomata, show several varieties. 2.
The commonest, and therefore most important, is that derived from soft nævi which
are endotheliomata of lymph-vessel origin. Nævomelanoma, whose histogenesis it
is not possible to determine, must be referred to the same origin. 3. A second variety
896 NEW GROWTHS
takes issue with the conclusions of these investigators, and joins the Ger
man general pathologists in support of the view that has generally been
held until recently, that the malignant growth, called by Unna melanocar-
cinoma, takes its origin from the lymphatic endothelium. Fordyce1
takes conservative ground, believing that there is still some doubt as to
the origin and nature of these growths, and prefers for the time the non-
committal name melanoma. In addition to the points of origin named,
melanotic sarcoma may originate in any pigmented spot in the skin,
although in some instances its source is not readily demonstrable. It

Fig. 224. — Melanotic sarcoma, starting in a mole—(Stelwagon-Gaskill, Jefferson
Hospital case).
not infrequently has its origin on the hands or feet, at the dorsal or lateral
aspects, sometimes the first evidence presenting being an easily abraded
exists with the same histologic pictures, which does not spring from nævi, and whose
origin is directly traceable to endothelium, probably also lymphatic. This group in
cludes melanotic whitlow and the malignant lentigo of the French. 4. The third di
vision is truly epithelial in origin, although its existence has been denied. These tumors
are of various types and show only a very slight tendency to malignancy, a fact suffi
cient in itself to determine a cardinal difference from the melano-endotheliomata, whose
capacity in this connection can hardly be exaggerated. 5. A histologic diagnosis is
the only proper method of differentiation between the two.
1 Fordyce, “Melanomas and Some Types of Sarcoma of the Skin,” Jour. Amer. Med.
Assoc, Jan. 8, 1910, p. 291 (with histologic cuts, review of the subject, and references);
Gibbon and Despard, “Melanotic Neoplasms,” Internat. Clinics, vol. iii, 18th series
(report of cases, review, and bibliography), also consider the matter unsettled; Gaskill,
“Melanotic Sarcomas Resulting from Irritation of Pigmented Nævi,” Jour. Amer. Med.
Assoc., Feb. 1, 1913 (reports an interesting case, with case and histologic illustrations,
brief review and references—case illustrated in the text).
SAKCOMA CUTIS 897
black superficial blister. Funk states that the initial evidence is some
times noted to be dilated capillaries or a purpuric spot, or its first step
may be the “melanotic whitlow” of Hutchinson, beginning, as this ob
server and also Duplay and Halle have described, as a pigmentation
around the border of a nail. The first changes in melanotic sarcoma
may be slow and insignificant, consisting simply of a dark-colored abra
sion with a smooth, irregular, or slightly fungating surface. Or there
may be an insignificant tumor growth, pea to small nut in size. In other
instances the early appearances, as in Stower’s1 case, involving the left
ear in a girl of eleven, consist of a slate-colored, a somewhat uneven and
verrucous area, or the patch may be smooth and slightly thickened.
Its course is rapid, general involvement soon ensuing, as illustrated by
a case under my care in a woman aged fifty; the development was ex
treme, numerous tumors not only in the skin, but also in the mouth,
throat, and eye, with a general discoloration of the skin and mucous
membranes, death ensuing from exhaustion within a year after the dis
ease first presented.
Multiple Pigmented (Hemorrhagic) Sarcoma.—The cases of this, the
third, class division made by De Amicis, are those known as multiple
pigmented sarcoma of Kaposi,2 who first described the disease upon
a basis of an observation of 5 cases, to which were later added others,
making a total in all of 25 patients. The number has been added to by
various other observers, among the earliest of whom Vidal, Wiggles-
worth, De Amicis (11), Semenow (10), Donner, Hardaway, Duhring,
Hallopeau, Funk, Schwimmer, and Mackenzie. In more recent years
reports of new cases have been made by Fordyce,3 Sherwell,4 Brayton,5
Magliano,6 Wende,7 Bernard,8 Sequeira,9 and others, so that the aggre
gate is becoming fairly large.
The malady, with rare exceptions, first presents upon the extremi
ties, and usually simultaneously. The beginning lesions may be small
nodular, discrete, aggregated, or crowded together, and scarcely exceeding
1 Stowers, Brit. Jour. Derm., 1803, p. 305.
2 Kaposi, Pathologie und Therapie der Hautkrankheiten, fifth ed., p. 922.
3 Fordyce, Jour. Cutan. Dis., 1891, p. 1, with colored plate; this and Schwimmer’s
case report (Internat. Atlas, 1889, ii, plate iv) give references to previous cases.
4 Sherwell, Amer. Jour. Med. Sci., Oct., 1892.
5 Brayton, Indiana Med. Jour., Nov., 1893.
6Magliano, Morgagni, May, 1894, xxxvi—abs. in Brit. Med. Jour., 1895, p. 196.
7 G. W. Wende, Jour. Cutan. Dis., 1898, p. 205 (with illustrations and histologic
cuts).
8 Bernard, Archiv, 1899, vol. xlix, p. 207 (2 cases with review of the literature).
9 Sequeira and Bulloch, Brit. Jour. Derm., 1901, p. 201 (case with colored plate
and brief review of subject, with numerous references). Some later reports: Bernhardt,
Archiv, 1902, vol. lxii, p. 237 (with references); Koehler and Johnston, Jour. Cutan.
Dis., 1902, p. 5 (with ease illustration and histologic cuts); Sellei, Archiv, 1903, vol.
lxvi, p. 1 (with plate and bibliography); Krzysztalowicz, Monatshefte, 1904, vol. xxxviii,
p. 215 (includes 2 cases—histologic); Parkes Weber and Daser, Brit. Jour. Derm., 1905,
p. 135; and histology of this case and histologic review, with references, by Macleod,
ibid., 1905, p. 173; Selhorst and Polano, Archiv, 1906, vol. lxxxii, p. 33 (1 case; male,
patient aged seventy; began when aged fifty; colored histologic illustration, and
partial bibliography); W. Pick, ibid., 1907, vol. lxxxvii, p. 267 (2 cases; with colored
plate case illustration, histologic cuts, and partial bibliography); Dalla Favera, Archiv.
1911, Bd. cix, p. 387, abs. in Brit. Jour. Derm., 1912, p. 82 (based on 6 cases, 3 dying;
autopsy; review of the subject; in 2 of the cases metastatic growths were found in the
internal viscera).
57
898
NEW GROWTHS
a pea in size. In some instances or in some areas, instead of distinct
tumor formation there is a thickening or diffused infiltration. In color
they may vary from a reddish-blue to a purplish color; on the lower
extremities a dark-brown shade or even a blackish hue may be observed.
The growths and areas of infiltration are generally of firm consistence,
and may be spontaneously painful, or more usually simply tender upon
pressure. Occasionally growths are observed somewhat suggestive of
angiomata, and which can be made smaller when firmly pressed upon.
In some tumors there may be a central depression, probably from partial
involution changes or relatively more active peripheral growth. Com
plete involution is noted at times in some growths, disappearing and
usually leaving a somewhat depressed, stained area or scar. Some, after
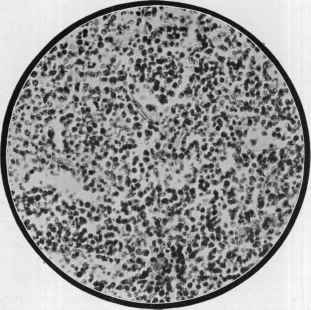
Fig. 225.—Small round-celled sarcoma (X 250) (courtesy of Dr. J. C. Johnston).
having lasted some months, may exhibit ulcerative tendency, but, as
a rule, this is exceptional, and only observed late in the disease. Dilated
capillaries around the nodules and interspersed are frequently seen.
The progress of the malady is a steady one, new growths and infiltration
being added from month to month; the legs, especially below the knees,
show much thickening and deformity, presenting a mild degree of ele
phantiasis-like enlargement. When well advanced, the general health
is gravely affected, the mucous membranes are invaded, and, according
to the findings of autopsies, the visceral organs are also sooner or later
involved. The average duration of the malady is, according to Kaposi,
whose experience is the largest, about four years; Favera makes the dura
tion eight to ten years, varying in the different cases from two to twenty
or more.
SARCOMA CUTIS
899
Etiology.—Possible etiologic factors have been casually men
tioned in describing the several varieties. The causes are yet to be
discovered. Beyond the effect of local irritation being an important
starting factor in some instances,—more especially the single non-
pigmented and melanotic varieties,—nothing is practically known.
Scarcely any age is exempt from the malady, although most cases are
probably seen under twenty and over forty.1
In multiple pigmented sarcoma no light has been thrown upon its
origin. It is almost wholly observed in males, and after the age of forty.
I have met with 2 instances of the disease, one a male, the other a female,
and both past middle life, the disease running a fatal course in four or
five years. All of Kaposi’s cases were males, and Sequeira (loc. cit.),
out of 73 cases in the literature, found a record of only 5 females, and
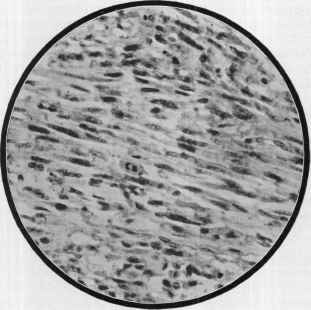
Fig. 226.—Spindle-celled sarcoma (X 250) (courtesy of Dr. B. H. Buxton).
was not sure that all of these were examples of the disease. His investi
gation disclosed also that most of the men were of powerful build. Ac
cording to Sequeira, in 3 instances the disease began after a chill; gout was
present in 4 cases, and rheumatism and valvular cardiac disease were
also observed in some instances.
Pathology.—The growths of the non-pigmented variety are
made up chiefly of round cells or mixed round and spindle cells. A
1 F. A. Packard, University Med. Mag., April, 1891, has reported a case of multiple
sarcoma (lymphosarcoma) cutis in a male infant of six months, beginning when aged
seven or eight weeks by the appearance of two or three pea-sized nodules of purplish
color on the back, the disease running a fatal course in six months.
900 NEW GROWTHS
case of a moderate number of tumors, observed by Crocker,1 in which
the early lesions were all excised, these were typical of alveolar sarcoma,
whereas the tumors which subsequently recurred were round-cell sar
comata. Hartzell also noted, in a case under his care of numerous sar-
comatous growths on the leg, that the histologic features of these tumors
bore but a faint resemblance to those of the growths which subsequently
appeared in the stump. In the cases associated with leukemia (leukae
mia cutis) and pseudoleukemia (quoting Fordyce), “the structure of the
tumors is composed of small round cells of the size and appearance of
white blood-corpuscles; in the early stage of development forming nodular
collections at the junction of the cutis and subcutaneous cellular
tissue.” Sarcomata of the spindle-cell and mixed type have also been
observed in leukemic subjects. Occasionally growths show a predomi
nant fibrous character (fibrosarcoma) or excessive lymphatic element
(lymphosarcoma) or the growths are made up of connective-tissue ele
ments, originating from the adventitia of the vessels, with conspicuous
development of new blood-vessels (angiosarcoma) .2 In melanotic sar
coma spindle cells and small and large round cells have been variously
observed, although generally the tumors are composed of spindle-shaped
cells. These growths have also been noted to be of the alveolar
type. The pigment, as already stated, is a product chiefly of the
neoplasm cells, the growths usually originating from normally pig-
mented tissue.
Multiple pigmented sarcoma, Kaposi (loc. cit.) states, is a round-cell
growth, except that in a few places the characters of spindle-cell sarcoma
are seen. The pigmentation is due to the capillary hemorrhages noted.
Other observers have found a predominance of fusiform cells—in For-
dyce’s examination arranged in bundles extending longitudinally, trans
versely, and obliquely, their transverse sections looking not unlike round
cells. Wende (loc. cit.) also found spindle-cell nests as a predominant
feature, Macleod, from his examination of Weber and Daser’s case,
clinically characteristic of the affection, states “that histologically it was
not a sarcoma, but a growth of organizing connective tissue cells asso
ciated with marked vascular dilatation, edema, and the deposition of
blood-pigment.” While its classification is not yet definitely decided,
it seems closer to the granulomata than to the sarcomata.
Diagnosis.—In the recognition of the various sarcomata the
history and course must be taken into consideration, and very frequently
a final opinion is possible only on histologic examination. A pigmented
nævus undergoing enlargement or showing irritation is suggestive as to
melanotic sarcoma, and when the case is advanced, the history of such,
together with the melanotic characters of the growths, will usually be
conclusive. The maladies ordinarily to be excluded are syphilis, granu-
loma fungoides, and leprosy.
1 Crocker, Diseases of the Skin.
2 Cases of somewhat varying character have been recently reported by Winfield
(Jour. Cutan. Dis., 1900, p. 113, with illustrations); Fordyce (Amer. Jour. Med. Sci.,
1900, vol. cxx, p. 159, with histologic cuts); Johnston, Jour. Cutan. Dis., 1901, p. 126
(with histologic cut); Wolters, Archiv, Sept., 1900, p. 269 (with histologic plates);
Spiegler, ibid., 1899, vol. 1., p. 163 (with colored and other cuts).
SARCOMA CUTIS
901
Prognosis and Treatment.—A fatal issue is to be expected
sooner or later in all cases in which generalization has taken place,
varying from a few months to several years or longer, depending upon
the variety and extent. The melanotic type is the most rapidly fatal.
The multiple pigmented form, usually the slowest in its course—Bray-
ton’s case over twenty-five years, and Taylor’s1 patient, with a number
of sarcomatous growths, was still in good health twenty-four years after
its first appearance, and Jackson’s2 case, twenty-one years. Rare ex
ceptions of final spontaneous recovery have been noted, the most re
markable of which was Hardaway’s3 generalized case, which, after
lasting for over ten years, entirely disappeared. In 2 cases observed by
Bazin and Funk (loc. cit.), of a somewhat peculiar variety of the disease,
complete involution took place.
Operative measures are usually the sole method in those cases in
which the tumors are single or scanty in number. The x-ray treat
ment has been credited with a favorable influence in exceptional instances.
It has sometimes been noted that excision of a melanotic sarcoma seemed
to spur the process onward.
Under treatment by arsenic, preferably employed subcutaneously,
several instances of cure and marked palliation have been observed,4
usually in the multiple pigmented variety. Lustgarten5 saw marked
improvement in a case of this type from x-ray treatment; and Wall-
hauser6 had an apparent cure in one instance, and temporary arrest
in another, with wet compresses of mercuric chlorid solution (1: 500).
The fact that some instances of recovery have followed accidental
erysipelas led to the somewhat dangerous use, by Coley7 and others,
1 Taylor, Arch. Derm., 1875, p. 307.
2 G. T. Jackson, Jour. Cutan. Dis., 1897, p. 473.
3 Hardaway, ibid., 1883, p. 97, with colored plate; ibid., 1884, p. 289; ibid., 1890,
p. 21.
4 Köbner (Berlin, klin. Wochensch., 1883, p. 21), case of a girl of eight and one-half
years, was wholly relieved by hypodermic injections of 2½ to 4 minims of freshly
prepared Fowler’s solution with 2 parts water, and was free from a return five years sub
sequently. Later (Berlin, klin. Wochensch., p. 193), owing to the difficulty of securing
freshly made solution, Köbner expressed a preference for a solution of sodium arsenate.
Sherwell (Jour. Cutan. Dis. (discussion), 1897, p. 141) states that a patient with mul
tiple pigmented sarcoma, the lesions mostly upon the lower extremities, got entirely
well under full and increasing doses of Fowler’s solution, and was well a year later
when last seen. This same observer (Amer. Jour. Med. Sci., Oct., 1892) also reported
a multiple case in which the involution of the lesions was markedly influenced, new
ones appearing as soon as the patient discontinued the remedy. Hyde (Hyde and
Montgomery, Diseases of the Skin, fifth edit.) also refers to a case exhibited at the In
ternational Dermatological Congress, London, 1896, in which the eruption on the hands
disappeared under this plan of treatment; De Amicis (Monatshefte, 1897, vol. xxv, p.
309) has reported 1 case cured and 1 greatly relieved; Lassar and Shattuck (both
cited by Wende, loc. cit.) have also had good results, and Wende’s case was showing
some favorable influence; Lustgarten (Discussion, Jour. Cutan. Dis., 1897, p. 83),
in a case of sternal osteosarcoma with axillary gland involvement in which a prominent
surgeon refused operation, saw a complete disappearance in three months under in
jection of sodium arsenite, administered in a 2 per cent, carbolic acid solution.
5 Lustgarten, Jour. Cutan. Dis., April, 1905, p. 171 (case demonstration).
6 Wallhauser, Jour. Amer. Med. Assoc, 1909, vol. liii, p. 1608.
7 Coley, “Treatment of Malignant Tumors by Repeated Inoculations of Erysipelas,
etc,” Amer. Jour. Med. Sci., 1893, vol. cv, p. 487, with analytic table and full bibli
ography and “Recent Cases of Inoperable Sarcoma Successfully Treated with Mixed
Toxins of Erysipelas and Bacillus Prodigiosus,” Surgery, Gynecology, and Obstetrics,
Chicago, Aug., 1911 (a favorable record).
902
NEW GROWTHS
of the induction of this lattter by injections of cultures of the strepto
coccus of this disease, and also by the combined toxins of this coccus
and the bacillus prodigiosus.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |