| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
Papular Syphiloderm (Synonyms: Papular syphilid; Syphilo-
derma papulosum; Syphilis cutanea papulosa).—There are several va
rieties of the papular syphiloderm, which, inasmuch as they differ ma
terially in clinical appearances, can be most conveniently considered
separately, under the heads of the miliary papular syphiloderm, flat pap
ular syphiloderm, and the papulosquamous syphiloderm.
Miliary Papular Syphiloderm (Synonyms: Miliary papular syphilid;
Acuminated papular syphiloderm or syphilid; Follicular syphiloderm
or syphilid; Syphilitic lichen; Lichen syphiliticus).—The miliary papular
syphiloderm is a tolerably common manifestation of secondary syphilis,
but much less so than the flat papular eruption. Other associated symp
toms of the active stage of syphilis are naturally usually to be found.
It may appear apparently independently of an earlier macular syphilid,
and most frequently between the third and fourth months. In contra
distinction from the flat papular eruption it is follicular—connected with
the hair-follicles. There are two varieties—the small miliary papular
syphiloderm and the large miliary papular syphiloderm, although there
is in reality but slight difference, and therefore the variety is not always
clearly defined. In the small miliary papular syphiloderm the lesions
are pin-head in size, in the larger form two or three times as large. They
may be acuminate or somewhat rounded. As a rule, the eruption comes
out rapidly, and continues to appear for several days or one or two weeks.
1 Schmidt (Archiv, Oct., 1912) reports an additional case, and briefly reviews
Ehrmann’s paper.
SYPHILIS
781
It is usually most abundant upon the shoulders, upper part of trunk,
arms, and thighs. It is also frequently in profusion upon the face.
The lesions are often closely crowded, with a tendency to form groups
and aggregations, this being especially shown in relapses or when the erup
tion appears rather late. In relapses they may also tend to form seg-
mental and circular grouping. At first they may be of a pinkish-red
color, but, as a rule, and always sooner or later, they are of a dull or
ham-red color, with a brownish or violaceous tinge, are solid and some
what rough to the touch, and in the larger lesions there may be slight or
scarcely perceptible central depression or umbilication. Generally,
however, they are somewhat acuminate or conic, often with a slightly
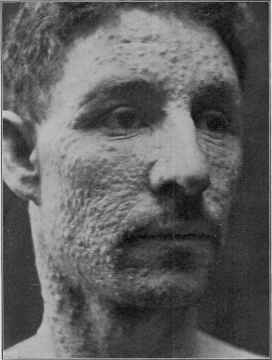
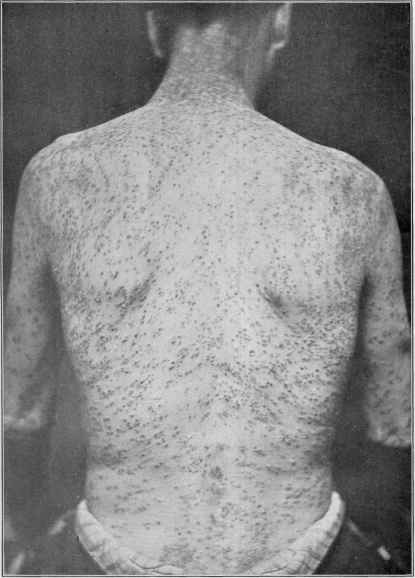
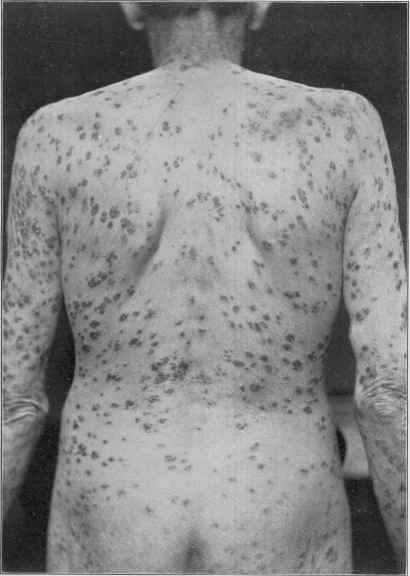
Fig. 177.—Papular and papulotubercular syphiloderm; eruption general.
scaly apex, and not infrequently show minute, vesicopustular or pustular
summits. In fact, it is not at all uncommon to see a slight or moderate
sprinkling of miliary pustules. There are sometimes also several or more
scattered flat papules, especially about the genitalia and anus, where
they frequently change into moist papules. After lasting for some weeks
or a few months there is a slight, sometimes moderately well-marked,
tendency toward spontaneous disappearance; the color becomes duller
or more somber, and especially as the papules sink away there is often
around the outer portion a collar or collarette of film-like scaliness.
The miliary papular syphiloderm is, as already intimated, somewhat
chronic in its course, and often persists for months, and is, when com
782
NEW GROWTHS
pared with the macular and flat papular syphilodermata, slow to respond
to. treatment. Those having vesicopustular or pustular summit show a
capping of brownish, thin, desiccated crusting. During its existence
it is not uncommon to see scattered fresh papules, and sometimes a few
pustules appear at irregular intervals. Like the others, there is rarely
any complaint of subjective symptoms, but in the negro there seems to
be considerable itching associated with this type. Minute brownish
stains marking the sites of the lesions are left for a variable period—
sometimes for months; there is no scarring, unless with pustular lesions,
which may leave insignificant atrophic or cicatricial points or pits.
The diagnosis of the miliary papular syphiloderm is to be based
upon distribution and extent of the eruption, the color, the tendency
to group and form aggregations, and the presence usually of some lesions
with pustular summits, often scattered minute pustules, and occasion
ally a few large papules and pustules; these features, together with the
existence of one or several associated symptoms of syphilis, will scarcely
permit of error. It is not to be confused with keratosis pilaris, psoriasis
punctata, pityriasis rubra pilaris, papular eczema, or lichen planus.
Keratosis pilaris is most pronounced and often limited to the thighs,
sometimes also on the arms, but rarely on the trunk; there is no crowding
or aggregation, it is often itchy, and usually already of long duration
when advice is sought, with but little tendency to spontaneous disap
pearance. The lesions of psoriasis in the earliest formation bear some
resemblance, but are not follicular, do not tend to form groups and aggre
gations, and are all scaly papules, with no pustular tendency, and the
distribution, while it may be more or less general, is usually most pro
nounced about the extensor surfaces of the legs and arms; it is chronic,
and commonly a history of long duration is given, and there is, more
over, a definite tendency to enlargement of the lesions into plaques,
which may become confluent. Pityriasis rubra pilaris is a scaly papular
follicular disease, but without disposition to pustulation, and with a
tendency to confluence, marked scaliness, and progressive, persistent
spread and chronicity. The marked itchiness of papular eczema, its
usually limited distribution and tendency to solid confluent patches,
the vivid red color, and often associated vesicles, will serve to prevent
mistake. Probably its strongest resemblance in some instances is to
lichen planus, but this latter is rarely generalized, favorite situations
being the lower part of the legs and forearms, to which it is often limited;
there is a decided tendency to confluence and solid scaly patch-formation;
it is usually slow in its advent and persistent, often slowly progressive,
and, as a rule, very itchy. The scattered aggregations of relapses may
suggest lichen scrofulosus, but this latter is a rare affection, usually
occurring as several, rarely more, livid or brownish papular aggregations,
of chronic, persistent character, and commonly associated with other
evidences of the scrofulous diathesis.
Flat Papular Syphiloderm (Synonym: Lenticular papular syphilo-
derm or syphilid).—The lesions vary in size from that of a pin-head to
a bean or larger. In some instances the eruption is made up entirely or
predominantly of papules scarcely larger than a pea, and. in others almost
Plate XXIII.
Miliary papular syphiloderm with a tendency in some lesions to become pustular at the
summit; shows the disposition toward small aggregations.
SYPHILIS
783
all the lesions are large—pea- to large coin-size—hence the two so-called
varieties—the small flat papular syphiloderm and the large flat papular
syphiloderm. The papules are flattened, often but slightly elevated,
rounded or ovalish in contour, dull or brownish red in color, and to the
touch often disclose considerable infiltration or depth, at least as com
pared to elevation above the surface. The lesions are generally dis
tributed, with but little tendency to closely crowded aggregations,
except in some cases of the small papular syphiloderm, in which the region

Fig. 178.—Small flat papular syphiloderm, of general distribution and extensive
development.
of the nose is a favorite site for some bunching, here partaking sometimes
of the nature of tubercles, being papulotubercular in character. Ordi
narily in the flat papular syphiloderm there is no disposition to coa
lescence, the lesions remaining discrete. The eruption is rarely so abun
dant as in the miliary papular syphiloderm, and, as a rule, there is less
tendency in this type to admixture of other forms, although sometimes
some macules or maculopapules and a few scattered pustules can be
found, and occasionally some miliary papules. The eruption is found
on all parts—scalp, face, trunk, and limbs; the flexor aspects of the last
784 NEW GROWTHS
usually show a preponderance over the extensor surfaces. The corners
of the mouth, the nasolabial folds, the forehead near the hair-border, the
palms, and the genitocrural and anal regions are favorite situations for
lesions. The irregularly arranged line of papules on the forehead, at
the hairy border, is commonly present in this and sometimes in other
forms of syphilitic eruption, and has been termed corona veneris.
This syphiloderm is a common one, and may be in some cases the
first recognized cutaneous eruption of syphilis, occurring usually several
or more months after the appearance of the initial lesion. In other
instances it follows after the macular syphiloderm—probably much more
frequently so than clinical experience would indicate, the macular erup
tion often being slight and readily overlooked. The eruption comes out,
as a rule, somewhat rapidly, although in some instances its full develop
ment is not reached for several weeks or more. Occasionally it is some
what scanty, the lesions being seen chiefly about the favorite regions.
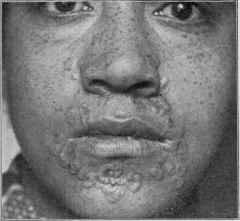
Fig. 179.—Annular syphiloderm.
In other cases they are merely a relatively insignificant, associated part
of a macular syphilid. At first the papules are perfectly smooth, some
times the surface slightly glossy, but later it is not uncommon for them
to become covered with a thin film of exfoliating epidermis.
While they are generally all rounded or oval in shape and persist
as such, with no tendency to special or peculiar configuration, excep
tionally, however, annular or distinct ring-like patches (annular syph-
iloderm, circinate syphiloderm) are observed, especially about the
region of the mouth, forehead, and neck, in association with the eruption
of ordinary rounded or oval patches on other parts. This lesion consists
of a distinctly elevated, solid ridge or band peripherally, and a more
or less flattened central portion. It seems to have its origin from an
ordinary, usually scaleless or slightly scaly, large papule, the central
portion of which has been incompletely formed or has become sunken
and flattened; and also from a spreading small papule, the central part
sinking or disappearing as it extends. It may doubtless occasionally
Plate XXIV.
Papular and papulosquamous syphiloderm.
SYPHILIS 785
develop from other lesions (Hazen), possibly may exceptionally arise
as ring-shaped lesions from the beginning. It is also seen occasionally
in association with the macular eruption, in which the band-like ring is
but slightly elevated. It is an unusual manifestation in the whites, but
not at all uncommon in the negro.1 In very rare instances the eruption,
especially about the face and scalp, may present as closely arranged
segments, sometimes of such elaborate arrangement or design as to sug
gest a resemblance to scroll work.
In most cases after several weeks or a few months they begin to de
cline, passing away by absorption, leaving slight pigmentation, which
eventually disappears. Not infrequently there is tendency from time
to time to less extensive outbreaks, and the eruption may thus persist

Fig. 180.—Annular syphiloderm (cour- Fig. 181.—Annular syphiloderm—
tesy of Dr. Howard Fox). showing scroll work tendency (courtesy
of Dr. Howard Fox).
for some months. As a rule, it responds rapidly to treatment, although
palmar and also plantar lesions are often obstinate, and on these regions
persistency and recurrence are frequently noted—palmar syphiloderm,
plantar syphiloderm. In some situations, moreover, as about moist,
contiguous surfaces, papules are apt to undergo certain changes, resulting
in the formation of the moist papule. These several forms will be espe
cially referred to later.
1 Howard Fox, “The Annular Lesions of Early Syphilis in the Negro,“ Archiv., 1912,
cxiii, with brief review, and excellent case illustrations; refers to previous papers on
the same subject by Atkinson, Jour, Cutan. Dis., 1883, p. 15; Gilchrist, Maryland Med.
Jour., 1909, p. 200, and his own earlier paper, “Observations on Skin Diseases in the
Negro,” Trans. VI, Internal. Dermat. Congress, 1907, vol. 1, p. 198. Hazen, “The
So-called ‘Annular Syphilis’ of the Negro,” Jour. Cutan. Dis., 1913, p. 148 (with illus
trations) .
50
786
NEW GROWTHS
In some cases of the flat papular syphiloderm there is a distinct
tendency, at times early in the eruption, at others later, toward scale-
formation, constituting the type known as the papulosquamous syph-
iloderm or syphilid (also termed syphilis cutanea squamosa, squamous
syphiloderm, or syphilid; and, from its resemblance to psoriasis, the
misleading and erroneous designation of syphilitic psoriasis, psoriasis
syphilitica, has sometimes been used). This tendency of the large pap
ular eruption to become scaly is, when exhibited, more or less common
to all the papules, although in some instances it is observed only here
and there. The papules usually become slightly less elevated, and are
covered with a dry, grayish or dirty-gray, somewhat adherent scale.
The scaling on some lesions is simply film-like and somewhat wrinkled,
in others more abundant; as a rule, as compared to that of psoriasis, it
is less imbricated, less shining or glistening, and relatively slight in
amount. If removed, the solid, flat, dusky-red colored papule is dis
closed. The eruption may be, as in the ordinary flat papular eruption,
general, as usually the case in the earlier months of the disease, or it
may appear as a relapse or a later manifestation, and be limited in ex
tent. As a late limited eruption it is most frequently seen on the palms
and soles, known commonly as the palmar and plantar syphiloderm.
The distribution in the generalized cases is the same as that of the more
usual papular syphiloderm, and is less abundant on the extensor than
flexor surfaces of the limbs, and there is, likewise, but little tendency to
coalescence. It is commonly more or less persistent for several months
or longer, although it usually responds fairly promptly to treatment.
There are no subjective symptoms, although in this papular syphiloderm,
occurring in the negro, as in other forms, itching is frequently compl ined
of.
In the diagnosis of the flat papular syphiloderm in the ordinary
or relatively scaleless forms there is rarely any dimculty. The more
or less generally distributed, variously sized, brownish-red or copper-
colored, flattened papules, showing infiltration, are characteristic; moist
papules are also usually to be found about the anus and genitalia. As it
is an eruption of the active or secondary period of syphilis, other cor
roborative symptoms will be found. The differentiation between the
papulosquamous syphiloderm and psoriasis is considered under the latter
disease.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |