| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
Palmar and Plantar Syp-hiloderm.—The palms (palmar
syphiloderm) and soles (plantar syphiloderm), especially the former,
are not uncommon seats of the dry syphilodermata—macular, macu-
lopapular, papular, papulotubercular, and tubercular. These parts
usually share in the more or less generalized eruptions of the active
or secondary stage of syphilis, but they are not infrequently alone the
sites of the relapsing secondary eruption, and often show the papulo-
squamous form at later periods of the disease. It is usually the latter
which furnishes the cases of the so-called palmar and plantar syphiloderm.
The thickness of the epiderm on these parts gives rise to considerable
modification; the lesions are but slightly elevated above the surrounding
SYPHILIS
787
level, are often rather ill defined peripherally, and when first appearing
are much more suggestive of macules than papules. There is some
elevation, however, and also distinct infiltration. They are rounded or
somewhat irregularly shaped, and in their early stage brownish yellow
or brownish red in color; later, owing to the collection of slight scaliness
or from being covered with dry, shriveled, broken epidermis, they are
dirty gray or grayish white, but when deprived of this covering, the
underlying surface or lesion has the usual brownish-red or ham color.
Not infrequently there is a slight central grayish or brownish-gray,
callus-like thickening, surrounded by a partly visible band of brownish-
red underlying papular infiltration, the color being disclosed by the partial

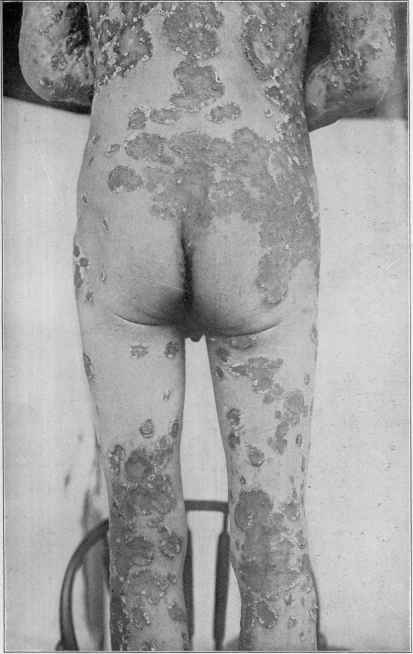
Fig. 182.—Flat maculopapular and papular syphiloderm. with scaling tendency;
generalized, the lesions on other parts being maculopapular, papular, and papulo-
squamous.
or more or less complete removal of the thin scale; beyond this an en
circling rim of partially detached epidermis, with its loose, elevated,
usually ragged edge directed inwardly. There is often a disposition
toward coalescence of contiguous lesions, and this results in the formation
of irregular, segmental, crescentic, and serpiginous patches or tracts.
This tendency, particularly the serpiginous and circinate, is observed
with the late papulotubercular manifestation, and such patches often
creep, with a slightly elevated spreading border, on to the fingers or
up the wrist, and not infrequently toward and sometimes over to the
dorsal surfaces of the hand and fingers. The general appearances of the
papulotubercular and tubercular forms differ but little from that of the
ordinary papulosquamous just described, the sole difference being that
788 NEW GROWTHS
the lesions are usually somewhat deeper and showing, as a rule, more
infiltration, and occasionally the tubercular exhibiting a slight disposi
tion here and there, at the spreading edge, to superficial ulceration.
The difference is so slight that, after the eruption is once established,
it is scarcely, if at all, recognizable; the spreading elevated infiltrated
edge with ulcerative tendency always, of course, indicates the papulo-
tubercular or tubercular syphilid.
In some cases there is a tendency to fissuring and the fissures may
be superficial or deep. The scaliness is, as a rule, scanty, more of the
nature of fragmentary, ragged, partially detached epidermis, and is
reproduced slowly. Occasionally, however, it may be more abundant,
and sometimes collects to slight thickness; it is noted to be quite hard
and horny. Now and then these hard, horny collections are small and
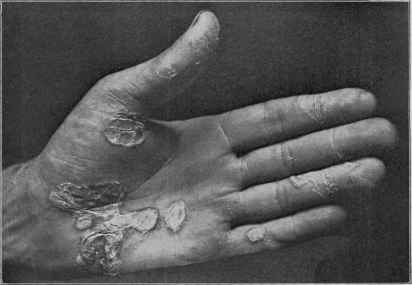
Fig. 183.—A papulosquamous syphiloderm, of the palm only; late eruption.
rather sharply circumscribed, extend somewhat deeply, and which can,
with some force, be dug out; sometimes they show sieve-like perforations;
the French writers called attention to this condition, which they de
scribed under the name of syphilide cornée. Exceptionally palmar and
plantar lesions remain more or less persistently as maculopapules or
papules, showing some epidermic thickening, with but little tendency to
scale-formation.
The eruption is sometimes observed on both palms and soles more or
less symmetrically; it may be scanty or abundant. More commonly
it is limited to the palms, and not infrequently to one hand. It may also
be confined to one or both soles. It is usually slow in its advent, spreads
gradually, but, as a rule, does not become extensive, sometimes remain
ing more or less stationary for an indefinite time. The central portion
SYPHILIS 789
of the palm, the ball of the thumb, and the volar surfaces of the fingers
are favorite situations on the hand. It is not itchy, but if fissuring is
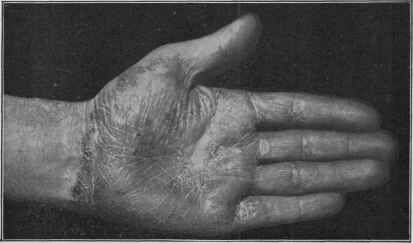
Fig. 184.—A palmar spreading papulo- and tuberculosquamous syphiloderm of the
late period, showing the well-defined border, leaving pigmentation and slight atrophy;
no eruption elsewhere.
present, is, for this reason, often painful; the process is sluggish, more of
the nature of an infiltration than inflammation, although it commonly,

Fig. 185.—A palmar papulosquamous syphiloderm of the late period; no eruption
elsewhere.
especially in spreading areas, presents on the parts traversed a reddish,
sluggishly or subacutely inflammatory aspect, sometimes with an ap-
790
NEW GROWTHS
pearance of thinning, and commonly scantily covered with adherent
and detached fragments of epithelial scales.

Fig. 186.—A palmar tuberculosquamous syphiloderm of the late period, showing seg-
mental configuration; no eruption elsewhere.
The palmar and plantar syphiloderm occurring late in the disease
is a persistent obstinate manifestation, and often extremely rebellious

Fig. 187.—A palmar papulotubercular spreading syphiloderm of the late period, with
ulcerative tendency, and showing the sharply defined border; no eruption elsewhere.
to treatment. As a part of a generalized eruption of the early or active
stage it disappears usually along with the eruption on other regions,
PLATE XXV.
Papulotubercular squamous syphiloderm ; undergoing involution (courtesy of Dr. M. B.
Hartzell).
SYPHILIS
791
although it may remain much longer on these parts, finally yielding
to remedies. As a recurrence of the early generalized type, and
limited to these regions, it is somewhat obstinate, but much less so
than when appearing several years or more after the contraction
of the disease. The papulotubercular or tubercular form, more
especially that with ulcerative tendency, is generally much more
readily cured.
The diagnosis of the palmar syphiloderm is often a matter of great
difficulty. It bears resemblance to eczema, dermatitis seborrhoica,
and possibly to psoriasis. As a part of an early generalized syphiloderm
a conclusion is naturally easily reached, but special reference is here
made to the eruption as found limited to this region. Psoriasis can,
I believe, be readily excluded by the fact that it is never limited to these
parts alone, but if found here, lesions will surely be found about the
elbows, scalp, and probably elsewhere. It is true, a few instances of
psoriasis confined to the palms have been reported, but such have been
so extremely rare, and inasmuch as the clinical appearances of psoriasis
of these parts, when seen exceptionally in connection with a generalized
psoriasis, are so much like some cases of eczema, especially dermatitis
seborrhoica, and even like palmar syphilis, that the alleged cases of
limitation to these regions could much more reasonably be placed to the
credit of either of the latter two maladies.
In fact, in the diagnosis only eczema and dermatitis seborrhoica
need be considered. Eczema can usually be differentiated by the more in
flammatory aspect, the common and often predominant involvement
of the fingers and finger-ends, and generally its appearance also on the
backs of the hands, as well as the presence of variable heat and itching;
often, too, there is present in one or two places the eczematous discharge,
or a history of such; there is no tendency to crescentic, serpiginous, or
circinate forms, as often observed in syphilis; and not infrequently it
occurs in those who have to do with irritating substances, as dyers,
plasterers, pasters, polishers, etc Sometimes, too, in such eczema
cases the eruption in its characteristic aspects is seen on forearms, and
possibly elsewhere. It is with the differentiation from dermatitis sebor-
rhoica, which, however, is luckily somewhat rare in this situation,
that the most difficulty is likely to be encountered, as itching and
burning are often absent in this malady, and it may show a slight
tendency to crescentic configuration. A careful consideration of both
diseases is occasionally necessary, sometimes supplemented by observa
tion and treatment, before a positive conclusion can be reached. Derma
titis seborrhoica is, however, much less likely to form segmental,
crescentic, and serpiginous shapes than syphilis, and with such as a pre
dominant feature the latter diagnosis would be the more probable unless
there were good reasons for the contrary. Dermatitis seborrhoica,
fortunately, is commonly associated with the same disease on one or
more of its more usual situations, as the scalp, eyebrows, nasolabial folds,
bearded region, interscapular and sternal regions; when on the hands, it
is usually long after it has already existed elsewhere. Moreover, in
dermatitis seborrhoica there is not the usually distinctly recognizable
792
NEW GROWTHS
infiltration of the syphilid. In many instances in these cases of palmar
and plantar syphilid often a history of syphilis is obtainable, or evidences,
such as scars, of former syphilitic manifestation can be found. Occurring
during the active or secondary period of the disease, of course, other
associated symptoms are commonly present, but when occurring a few
years or longer after the contraction of the malady, such positive cor-
roboration is generally wanting. In urgent cases the Wassermann test
might be a help.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |