| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
5. LUPUS VULGARIS
Synonyms.—Lupus; Lupus vorax; Fr., Lupus vulgaire; Lupus tuberculeux; Scrofu-
lide tuberculeuse; Ger., Fressende Flechte.
Definition.—A chronic cellular new growth, due to invasion of
the integument by the tubercle bacillus, characterized by variously sized,
soft, reddish-brown tubercles, tubercular and infiltrated patches, usually
terminating in ulceration and scarring, sometimes in absorption, exfolia
tion, and atrophy.
Symptoms.—The most common site for the manifestation of
the malady is the face, especially the region of the nose, although other
parts of the surface are not infrequently invaded either conjointly with
the face or independently. This will be referred to again. The disease
begins by the development of several or more pin-head to small pea-
sized, deep-seated, brownish-red or yellowish macules (lupus maculosus)
or small discrete infiltrations or tubercles, having their seat in the deeper
part of the corium, and which are somewhat softer and looser in texture
than normal tissue. As the disease progresses, usually, however, very
insidiously and slowly, by new lesions or infiltration at the bordering
part, a variously sized patch, consisting of crowded or aggregated tuber-
720
NEW GROWTHS
cles, results. The earlier nodules or infiltrated points, having attained
a certain size or development, about that of a small pea, remain sta
tionary, for a time at least, and then, sooner or later, exhibit retrogressive
changes and tend to break down and disintegrate, and destruction
results, terminating in ulceration. These latter are rounded, shallow
excavations, with soft and dark-reddish or brownish-red borders, and
with a variable amount of purulent secretion, but usually slight in
quantity, which leads to more or less crust-formation. Later, as the
patch gradually increases in area, the ulcerations are disposed, as a rule,
to heal, and finally give place to cicatricial tissue, generally of a firm
and fibrous character. The patch spreads by the appearance of new
papules or infiltrations at the peripheral portion, and not infrequently

Fig. 161.—Lupus vulgaris in a girl of fifteen, of six years’ duration.
new islets arise just outlying the border; the intervening space is gradu
ally filled up by other lesions, and the whole area becomes continuous.
In a typically developed patch of lupus, in which, as more commonly
noted, ulcerative tendency is observed (lupus exedens; lupus exulcerans),
several conditions are to be seen, even when the area is scarcely larger
than a silver quarter: the characteristic soft, small, yellowish or reddish-
brown (of apple-butter color and appearance) cutaneous and subcuta
neous points and papules; similarly colored or yellowish-brown tubercles
and infiltrations; ulcerations, usually small, rounded, and shallow,
sometimes confluent and irregularly shaped; cicatricial formation, which,
as a rule, is rather tough and keloidal; and, in addition, outlying the
involved area, but close to the border, can often be seen a few isolated
TUBERCULOSIS CUTIS
721
small infiltrated points or tubercles. These various lesions show the
several stages of the process from the beginning cellular deposit to the
resulting necrosis and cicatrization. So the disease continues, often
apparently remaining stationary for months or longer, so that in many
instances, and especially as met with in our country, several years or
more may have elapsed before the area involved is more than 1 or 2
inches across—usually irregularly shaped, although, as a rule, somewhat
rounded or ovalish. In other cases, instead of resulting in necrosis and
ulceration, the matured or oldest papules or tubercles or infiltrated patch,
after long continuance, slowly disappear, chiefly by absorption, fatty
degeneration taking place, and partly by exfoliation, leaving an exfoliat
ing, atrophic, or thin, cicatricial, pigmented tissue, constituting the clin-

Fig. 162.—Lupus vulgaris; chiefly of the exfoliative type, with pigmentation and
atrophic scarring; showing, as a result, ectropion; ulcerative action on other cheek.
Patient aged thirty-five; duration twenty years.
ical variety known as lupus exfoliativus. And in this way the disease
continues, presenting the various stages and lesions noted in the ulcera
ting form, except the ulceration and tough fibrous scar-formation. It is
not uncommon, both in the atrophic and scar tissue resulting from the
earliest lesions, for new foci of disease to appear from time to time, usually
isolated, and with very little tendency to confluence.
The disease may be more or less pronounced in one or more of its
features. In exceptional instances the ulcerations may be the seat
of exuberant granulations, and the underlying inflammatory and cellular
infiltration and edema be quite considerable or extreme, and with the
resulting cicatricial formation giving rise to hypertrophic disfigurement
and distortion—lupus hypertrophicus. In some cases, while in most
46
722
NEW GROWTHS
respects the disease is as usually observed, the cicatricial development
is hypertrophic, tough, and thick (lupus sclerosus); or there may show
itself a distinct keloidal tendency in the resulting scar tissue (lupus
keloides). In some instances the ulcerations become the seat of papillary
elevations or hypertrophy, and there is then presented a somewhat
uneven, papillomatous, exuding, and crusted surface—lupus papilloma-
tosus, lupus verrucosus. As the disease gradually advances the border
of tubercles or almost continuous infiltration may be irregular or tor
tuous, the innermost part showing the usual scar or atrophic tissue,
and the whole configuration and manner of spread be of serpiginous
character (lupus serpiginosus), somewhat closely resembling the ser-
piginous tubercular syphiloderm; and in cases with this tendency, as a

Fig. 163.—Lupus vulgaris in a youth of sixteen, of five or six years’ duration.
rule, the lupus infiltration and ulceration go almost hand in hand, so that
sometimes a rather large, pigmented, atrophic or tough cicatricial area,
with an infiltrated, ulcerating, irregular, or serpiginous border, is pre
sented. The various other terms sometimes used in connection with the
disease, such as lupus planus, lupus nodosus, lupus elevatus, lupus tumidus,
lupus œdematosus, lupus elephantiasicus, etc, are self-explanatory, signify
ing merely the accentuation or undue development of some special feature.
When the nose and immediate region are the parts involved, the
tissue, except cartilage, of this organ, especially at and about the end,
is gradually destroyed and changed into a firm, irregular, and thin
cicatrix, producing considerable deformity, the resulting contraction
often narrowing the nasal outlets. In other cases the atrophic thinning
and cicatricial tissue may tend to distend the nostrils. In occasional
TUBERCULOSIS CUTIS
723
instances, however, of lupus involving the nose the earlier tubercles or
infiltration give way to ulceration and then become the seat of papillo-
matous vegetations or hypertrophic granulations, resembling the same
type of syphilis very closely, as in a few instances under my own care;1
later scarring and the usual disfiguring changes result. Zeisler2 records
a somewhat similar case. When the spreading disease encroaches toward
the eye, the cicatricial formation which ensues frequently draws upon
the eyelid and produces moderate or marked ectropion. Involving or
spreading on the upper lip, often considerable edematous infiltration is

Fig. 164.—Lupus vulgaris of many years’ duration. (Stelwagon-Gaskill Jefferson
Hospital case.)
noted, the part assuming large proportions (lupus hypertrophicus).
Ordinarily, however, the usual features are presented, and with the con
sequent tough, often keloidal, cicatricial ending, the mouth is drawn,
sometimes slightly puckered, and the opening inconveniently narrowed.
Both when implicating the lip and the nose, the invasion of the nasal
1 Stelwagon, “A Somewhat Unusual Case of Lupus Ulceration of the Nose,” Jour.
Cutan. Dis., 1892, p. 428.
2 Zeisler, “Remarks on Tuberculosis of the Skin,” North Amer. Practitioner, March,
1889 (a clear and terse review, with many references).
724
NEW GROWTHS
mucous membrane, and even that of the mouth, is frequently observed,
and, indeed, the disease often starts from within the nasal orifice.
In some cases of lupus of the face, as well as when seated elsewhere,
not infrequently new foci appear one or several inches or more from the
original patch; or the disease may develop at several points simulta
neously, or one follow closely after the other. As a rule, however, and
especially as observed in our own country, there are but one or two
areas, which may be quite small and scarcely progressive, or exceptionally
extensive and involve a greater part of the face. In addition to the
disease presenting on the face, foci sometimes develop elsewhere on the
general surface, usually conjointly or subsequently to the face manifesta
tion. While, however, the face is the sole seat of the malady in most
patients, and commonly shares in the disease in instances in which the
eruption is noted on other parts, still there occur cases, not often, it is
true, where the eruption develops on the leg, arm, neck, trunk, or about
the genitalia, and remains limited to its original region, the face remain
ing free throughout. Bender,1 in an analysis of 374 cases, found that the
face was the seat of the disease in 287, of which, in 115, it was more or
less of the entire face; in 70, it was in the nose; 35, on the cheek; 25, nose
and other parts of face; 16, on lips; 15, nose and lips; 6, temple and fore
head; 3, chin; and 2, eyelids; 40, upper extremities; 15, lower extremities;
12, face and neck; 6, face and extremities; 3, face and arm; 3, ear; 2,
general; 2, scalp; 1, hand and foot; 1, nape of neck; 1, back, and 1, palate.
It presents no special peculiarities in the various unusual localities, ex
hibiting primarily the beginning maculopapular, yellowish-brown papules
or tubercles, closely aggregated or contiguous and confluent, and
progresses in the ordinary manner and with the same changes. There
seems to be a greater tendency shown on these regions for the malady
to be serpiginous in character, often exhibiting a close resemblance to
the serpiginous tubercular syphilid. In these cases, too, the exfoliative
feature is often more pronounced than it is usually upon the face. In
most the disease is limited to one region, although it often involves a
great extent of surface. The ulcerative tendency, when present, is
often quite pronounced, and if the disease is about a joint, may result
in serious deformity and materially restrict the mobility of the part.
When on the lower part of the leg and also about the genitalia and anal
region, the ulcerations are often the seat of papillomatous vegetations
(lupus papillomatosus, lupus verrucosus), with crusting and offensive
discharge; considerable thickening and edematous infiltration with
lymphangitis are also frequently noted with the disease when on the
extremities.
Lupus of the mucous membranes has been incidentally mentioned
in connection with that of the lip and nose, but the involvement may
also be conjointly with the disease some distance from these parts.
In fact, it is not improbable that in many cases of cutaneous lupus the
primary infection is within the nose. And cases of lupus invading the
throat are also recorded from time to time, though few in number, in
1 Max Bender (Ueber des Beziehungen des Lupus vulgaris zur Tuberkulose),
Deutsche med. Wochenschr., 1886, p. 413.
TUBERCULOSIS CUTIS
725
which there is no evidence of the eruption upon the integument. It
may consist of an insignificant or moderate diffused infiltration, with
slight papular or tubercular elevations, or more the nature of papillary
excrescences; or the area is studded with whitish epithelial opacities.
Superficial ulceration is not uncommon, and may assume a serpiginous
configuration; or it presents the aspects of a raw granulating patch.
The most commonly involved site is that of the nares, near the outlets,
and the mucous membrane of the inside of the lips, contiguous to the
adjacent skin. In most of these cases the disease has progressed from
the skin, although, as already stated, the primary involvement may
doubtless not infrequently be on the mucous membrane. Other parts,
such as soft palate, velum, hard palate, etc., may also be the seat of the
malady. According to Finsen,1 in the cases of lupus treated at his light-
institute, in 70 to 80 per cent, the mucous membrane of the nose or mouth
was also involved, a surprisingly large proportion when compared to
average American experience, and much, I feel sure, above that generally
observed. Bender,2 in 380 cases, found in about 45 per cent. (173 cases)
mucous membrane involvement conjointly with the skin; in 6 cases only
was the disease limited to the mucous membranes. In 147 of these 173
cases in which inquiry was made as to place of beginning it was elicited
that in 46 cases, or 31.2 per cent., the mucous membrane was the part
originally attacked. While in a number of instances but one mucous
surface was invaded (nose, 75; tear-duct, 9; conjunctiva, 8; lips, 12;
palate, 11), in many several regions were the seat of the disease, so that
in tabulating, the mucous membrane of the nose was found implicated
in 115 cases, conjunctiva in 21; tear-duct in 24; lips in 43; palate in 31;
tongue in 1; larynx in 13; rectum and vulva in 1.
While in the very large majority of lupus patients the usual char
acters and location are observed, occasionally atypical cases3 especially
as regards distribution, configuration, extent of eruption, and association
with other forms of integumentary tuberculosis present. A rare form,
usually on the face, but sometimes on other parts, is that described by
Leloir4 as lupus vulgaris sclerosus erythematoides, which resembles
closely and simulates lupus erythematosus (also referred to under this
latter disease). It is very slow in its course, tending to spread in a cen
trifugal manner, and never ulcerates. It is of a bright or dusky red color,
disappearing partly under pressure, and here and there, especially periph
erally, covered with fine scales or small lamellated crusts; somewhat
raised at the border, and slightly depressed centrally in consequence of
the tendency to atrophic cicatrization or interstitial resorption. If the
1 Stelwagon “An Account of a Visit to Professor Finsen’s Light-Institute at Copen
hagen,” University Med. Mag., Philada., Dec, 1900.
2 Max Bender, “Ueber Lupus der Schleimhäute” (a review of the literature with
references), Archiv, 1886, vol. xx, p. 892. See also valuable paper by Doutrelepont,
“Ueber Haut- und Schleimhauttuberculose,” Deutsche med. Wochenshr., 1892, p. 1033.
3 Howard Fox, “Three Unusual Forms of Cutaneous Tuberculosis,” Jour. Cutan.
Dis., Feb., 1912 (with illustrations); extensive case of lupus serpiginosum of somewhat
rapid development, strongly suggestive clinically of syphilis; case lichen-planus-like
inner aspect of thigh and knee; and a case with two tuberculous ulcerations, upon the
central portion of the mucous membrane of the lower lip.
4Leloir, Jour. mal. cutan., 1891, p. 241; good abstract in Brocq’s letter, Jour.
Cutan. Dis., 1892, p. 27.
J26 NEW GROWTHS
involved skin is put upon the stretch, as a rule small miliary tubercles of
a yellowish color become visible; there is a good deal of underlying infil
tration, which also distinguishes it from lupus erythematosus. Histo-
logic and bacteriologic findings and experimental inoculations proved
its tuberculous nature, although it presents clinically a meeting-ground
between these two affections. Hardaway1 believes this form much more
common than generally thought, but that it is usually confounded with
lupus erythematosus, a view which I am inclined to share. Very excep
tionally lupus patches from the start display a tendency to circinate
shape, with clearing, usually atrophic or cicatricial center, in some re
spects resembling, in shape more especially, the lupus vulgaris erythema-

Fig. 165.—Lupus vulgaris involving the entire face, scalp anteriorly, and the ears;
there is also a tubercular patch on the upper part of the arm; many years’ duration,
slowly progressive (courtesy of Dr. L. A. Duhring).
toides of Leloir, except that the borders are distinctly nodular. It begins
as a nodule, and this sinks centrally as it spreads. A rare instance of this
form—of added interest on account of the large number of such areas,
all of the same characters, varying in size from a pea to a dime or slightly
larger, and chiefly about face—is recorded by Elliot,2 which could be well
described by the name lupus annularis. In other cases, somewhat rare,
the eruption, instead of being limited to one or two regions or areas, is
quite generally distributed (lupus disseminatus). Crocker refers to a
case, a boy aged ten, in whom there were 47 variously sized patches
1 Hardaway, Manual of Skin Diseases.
2 Elliot, Jour. Cutan. Dis., 1896, p. 476; Ransom, ibid., 1895, p. 269, and Sutton,
ibid., 1910, p. 391, have each also reported an example; in each case but a single patch.
TUBERCULOSIS CUTIS
727
scattered over the whole body; and Morrow,1 a case, a woman of twenty-
two, in whom the disease developed some years previously, exhibiting,
with some caseating glands, various plaques of extensive distribution;
and Fordyce,2 in a man aged twenty-eight, in whom it had first appeared
at the age of four, and involved the whole face and neck; with numerous
patches over the arms, chest, back, etc Some years ago, when associated
with Professor Duhring, I saw in his clinic a case of a Hungarian woman
of twenty-one in whom a large part of the entire surface was involved,
on the legs the disease forming one continuous covering, with, however,
but little tendency to ulceration; and also recall several instances of
almost universal distribution in the clinics of Hebra, Neumann, and
Kaposi during my student days in Vienna. Such cases are, however,
extremely rare in our own country; less so in the European capitals.
In rare instances a verrucous or papillomatous tendency is noted in cases
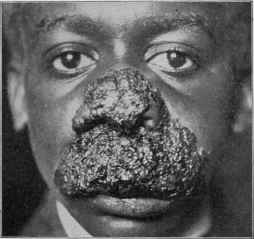
Fig. 166.—Lupus (tuberculosis cutis) of papillomatous type; in a negro youth of
eleven; duration two to three years; yielded almost completely to x-rays.; later
relapsing and spreading, patient finally, after several years, dying of pulmonary tuber
culosis.
showing scattered patches, with but few or no typical lupus nodules,
closely allied to or identical with tuberculosis verrucosa cutis.
In other instances lupus vulgaris areas are found associated with
various other tuberculous integumentary lesions and other signs of
tuberculosis. White3 briefly details 10 such cases, which had been
under his direct care, in which one or more clinical forms of tuber
culosis were present in association with lupus vulgaris, such as case-
ating and ulcerating glands, tuberculosis verrucosa, tuberculous dac-
tylitis, etc Wickham4 relates a case in which three forms were
1 Morrow (case demonstration), ibid., 1895, p. 259.
2 Fordyce (case demonstration), ibid., 1900, p. 119.
3 J. C. White, “ Clinical Aspects and Etiologic Relations of Cutaneous Tubercu-
losus,” Boston Med. and Surg. Jour., Nov. 12, 1891, p. 509 (an excellent presentation
and review of the subject).
4 Wickham, Paris letter, Brit. Jour. Derm., 1890, p. 337.
728 NEW GROWTHS
present: lupus vulgaris on face, tuberculosis verrucosa cutis on hands
and feet, and these two forms
about one knee, and tuber
cular abscesses—tuberculosis
gummata—on face and hands;
and Brousse and Ardin-Delteil1
had under observation a some
what similar case, a girl aged
sixteen, in whom the cutaneous
lesions, following a disease of
the bone of the right toe
when aged four, consisted of
a tuberculosis verrucosa cutis
of the right foot and leg, an
area of lupus vulgaris on the
left cheek, and a tuberculous
gumma of the side of the face.
W. G. Smith2 describes an un
usual case in which lupus of
the ordinary type was seated
about the nose, symmetric
exostoses on nose and lingers,
and on the latter also pulpy
nodosities, and a psoriasis-like
eruption on the body and
limbs, apparently leaving
scars; the true nature of this
last was obscure. In rare in
stances, however, the lupus
lesions do present a psoriatic
aspect, designated by Hutch-
inson lupus-psoriasis. Colcott
Fox3 recently recorded an ex
ample of this variety in a girl
under three years in whom
there were two patches on the
left knee and three on the
right; three on each buttock,
very closely symmetric; one
on the point of left elbow;
one on the back of right heel;
three on dorsum of left hand
and fingers; and one on the
back and on the flexor aspect
of the right wrist, and one on
right thumb; the bilateral, and to some extent symmetric localization, and

Fig. 167.—Lupus vulgaris of extensive
development; areas on nose, ears, trunk, and
thighs (courtesy of Dr. M. B. Hartzell),
1 Brousse and Ardin-Delteil, La presse méd., 1898, No. 32, p. 189
2 W. G. Smith, Brit. Jour. Derm., 1897, p. 187.
3 Colcott Fox, ibid., 1898, p. 329 (case demonstration).
TUBERCULOSIS CUTIS
729
the size and character of the patches simulating psoriasis. In these rare
cases, however, there is usually greater and denser infiltration, with well-
defined and infiltrated edges, than observed in this latter disease. Sooner
or later, as a rule, there is atrophy or scarring, and sometimes ulcerative
tendencies develop, as in a patient under my own observation, a young
girl aged eight, in whom the lesions, seated about the neighborhood of
both knees, were scaly and psoriatic in general appearance, although
tending to crowd together; several years later these gave place to ulcera-
tions of scrofulous aspect, and also simulating those observed in erythema
induratum and in syphilis.
The neighboring lymphatic glands in lupus cases, if of any extent,
sometimes, although not frequently, show inflammatory swelling and
enlargement, and tend to break down and suppurate, but, as a rule, this
is observed only in those instances in which ulceration is a feature, and
often due, doubtless, to the added pyogenic factor in the case. It has
been shown by Leloir,1 however, that in addition to adenitis due to in
flammatory products there is gland involvement due to direct tubercu
lous infection or transference from the lupus area; in 7 cases examined
by him this was established both by microscope and inoculation ex
periments.
There are no constitutional symptoms in lupus, unless from an asso
ciated internal tuberculosis; the occasional and probably, one might say,
frequent occurrence of other tuberculous processes, usually of the lungs,
noted will, as is to be expected, give rise to some general symptoms.
Lespinne2 has observed infective intoxication occur at times, with rise
of temperature, etc., and some suspicious pulmonary signs, due, he con
siders, to the absorption of the products of the bacilli; from which,
however, as a rule, no organic disease results; during such attacks he has
further noted that the lupus patch shows some reactionary symptoms
similar to those observed after tuberculin injection.3
The course of lupus has already been inferentially stated. It is
almost invariably a slow disease, appearing insidiously and from week
to week or month to month with scarcely perceptible progress. Fre
quently it develops gradually, but often with periods of apparent quies
cence, into a variously sized patch of a dime to that of one several inches
in diameter, and then remains stationary for a time; from occasional
partial subsidence of the inflammatory element retrogression some
times seemingly, and possibly with certainty, is observed now and then,
but, upon the whole, the malady gradually extends, showing no tendency
to disappear. Its presence, as a rule, gives rise to but little trouble
beyond its disfigurement, subjective symptoms being practically absent,
or not sufficiently annoying to give rise to complaint; the ulcerations,
especially when a decided pyogenic character is added, sometimes are
1 Leloir, abs, of paper, ibid., 1890, p. 55.
2 Lespinne, Jour. mal. cutan., Oct., 1891, p. 531.
3 Gaskill, ‘‘Extensive Tuberculoses Cutis with Death from Pyemia,” Jour. Cutan.
Dis., May, 1913, records an interesting case of wide distribution—chiefly face, lower
lumbar region, buttocks, and legs—of lupus vulgaris type, in which at intervals of
weeks or several months, there developed diffused, somewhat superficial and flat, un
dermining abscess-like formations; death finally resulted from pyemia.
730
NEW GROWTHS
painful and sensitive. Enlarged, swollen, and inflamed and caseating
glands may result in some cases, and general tuberculous infection may
eventually ensue. As we see the disease here, however, and for the most
part elsewhere, the patients are but little disturbed in a general way by
the presence of the local tuberculous process. Occasionally, it is true,
the open lesions seem to favor the development of erysipelas; and later
in life, in some instances, an epitheliomatous degeneration sets in, and
the malady then acquires a more serious character, especially as lupus
tissue seems to permit of rapid epithelial involvement and destruction,
often of a malignant type. Dubois-Havenith1 in 118 cases noted this
latter development 5 times. This is above the average proportion,
as it is generally believed to be between 1.50 and 2 per cent.
Etiology of Cutaneous Tuberculosis.—The disease, more
especially the ordinary type—lupus vulgaris—to which most of these
remarks apply, is common in some parts of the world—as, for example,
in Austria—and somewhat infrequent in others—as, for instance, in
our own country. The reasons for this are not perfectly clear, although
doubtless it is mainly to be found in the different methods of living,
the character of the food-supply, and other causes not known. Great
Britain also furnishes a large number of cases compared to this country.
The worst cases in this country, moreover, are usually found among the
foreign-born population. It is much more common in females than
males—at least two or three to one. It usually has its beginning in the
first periods of life, as in childhood and early adolescence; to this, how
ever, there are exceptions, although it is rare to see it beginning after
middle age. In Colcott Fox’s2 analysis of 96 hospital cases under his
observation, more than half began before the age of ten, and 30 of these
under five, and of the latter, 5 in the first year; 10 began after the thirtieth
year, and of these, 4 after the fortieth. Of the 96 cases, 64 were females.
Tuberculosis verrucosa and tuberculosis ulcerosa are often first seen later
in life, and exceptionally lupus may begin at that period.3
The direct cause of the disease, as first demonstrated by the find
ings of Demme, Doutrelepont, Pfeiffer, and Koch, and since by many
1 Dubois-Havenith, Du lupus vulgaire, Brussels, 1890 (an exceedingly valuable
monograph with a good review of etiology, pathology, and treatment).
See also the excellent monograph, Epithéliome et Lupus, by Desbonnets, Paris,
1894 (contains a review of reported cases); also Hutchinson’s paper, “Notes on Cancers
and Cancerous Processes,” Archives of Surgery, 1890-91, vol. ii, p. 138 (details several
cases of his own and refers to 6 cases observed by others); Sequeira, “Lupus Car
cinoma,” Brit. Jour. Derm., 1908, p. 40, besides giving his experience (1.5 per cent.)
in the London Hospital, reviews the subject (with bibliography); he is of the belief
that x-ray treatment, especially when the exposures are frequent and carried out over
long periods, tends to increase the proportion of instances in which epithelioma develops
on lupus vulgaris or its scars; Bargues, “Del’ èpithéliome sur lupus vulgaire,” Annales,
1910, p. 3, reports 6 new cases of epithelioma and lupus vulgaris from Dubreuilh’s
clinic, and gives an analysis of 164 published cases, and a tabulated review of these
cases, with full bibliography; Zweig, Archiv, 1910, cii, p. 83, adds 6 cases.
2 Colcott Fox, “On the Nature of Lupus Vulgaris from a Clinical Standpoint,”
Westminster Hospital Reports, 1893, p. 23.
3 See papers by Colcott Fox, “ Four Cases of Senile Tuberculosis of the Skin,”
Brit. Jour. Derm., 1892, p. 160, and by Travers Smith “Lupus and Senile Struma,”
ibid., p. 163. Colcott Fox refers to several contributions on the subject.
TUBERCULOSIS CUTIS
731
others, is the tubercle bacillus, a view which already had much support
in the clinical association with other tuberculous processes. In fact,
the clinical evidence of its tuberculous nature is today sufficiently large
to be in itself convincing. Bender1 found in 159 cases in which inquiry
was made, there were 99 (62.3 per cent.) patients in whom present or
past evidences of tuberculosis existed; hereditary predisposition was
noted in 33.3 per cent.; and at the time of examination in 77 cases other
signs of tuberculosis were present; 2 of his cases, while under observation,
died of other forms of the disease—1 of laryngeal and pulmonary tubercu
losis, and the other of tuberculous meningitis combined with caries of
the petrous bone. Colcott Fox in his series also noted the frequency of
family history of consumption, and in 33 of the 96 cases there were
evidences of the existence of glandular disease of some kind; 16 per cent,
of the patients suffered at some time from scrofulous gummata. In
Block’s2 144 cases 114 were affected with some form of tuberculous dis
ease, either prior to the attack (about 28 cases) or following it. In the
series reported by Sachs,3 out of 115 patients there were only 15 in whom
no past or present or hereditary tuberculosis could be found.4 Single
reported examples suggestive of its tuberculous origin are innumerable.
A striking one is that referred to by Walsh,5 of a young woman with
lupus upon the face and other tuberculous symptoms, whose father died
of phthisis, her mother of bronchitis, and eight or nine brothers of pul
monary tuberculosis. Winfleld6 records a case of a subject with pul
monary tuberculosis, in whose wife and daughter lupus developed.
Howe7 has also reported some suggestive examples. Such instances,
often less striking, it is true, are common in the experience of all ob
servers, and dermatologists of the present day are in accord as to their
significance.
Further evidence is to be found in examples of contagion or acci
dental inoculation and also in the success of experimental inoculation.
Several of the former may be referred to. White8 has observed a number
of cases in which lupus was presumably due to the inoculation of tuber
culous matter, 12 cases within a period of three years. Corlett9 also
met with such an instance; Jadassohn10 records 2 cases, 1 from a tubercu
lous ulcer and the other from a phthisical tattooer; Dent11 observed 3
cases of the disease develop in three sisters who slept in the same room,
1 Max Bender, Deutsche med. Wochenschr., June 17, 1886.
2 Felix Block, Archiv, 1886, vol. xiii, p. 201 (also gives the age at which disease
began, as well as regions affected, practically similar to the observations made by Ben
der and Colcott Fox).
3 Sachs, ibid., p. 241.
4 See interesting paper by J. C. McGuire (“Lupus Vulgaris: Its Relations to Tuber
culosis”), Jour. Cutan. Dis., 1891, p. 264, with review of this question, and interesting
replies concerning it from various authorities; also Payne’s address on Lupus, full abs.
in Brit. Jour. Derm., 1891, p. 369.
5 D. Walsh, Brit. Jour. Derm., 1898, p. 19 (case demonstration).
6 Winfield, Jour. Amer. Med. Assoc, Dec 12,1896, p. 1220 (with illustrations).
7 Howe, “Thirteen Cases of Tuberculosis of the Skin,” Jour. Cutan. Dis., 1892, p.
303.
8 J. C. White, loc cit., cites other cases from literature.
9 Corlett, ibid., 1893, p. 146.
10 Jadassohn, Virchow’s Archiv, 1890, vol. cxxi, p. 210.
11 C. J. Dent, Brit. Jour. Derm., 1891, p. 156.
732
NEW GROWTHS
while the other eight children of the family were free—the malady appar
ently originally arising from a pre-existing tuberculous ostitis in one of
the patients. Wild1 has recently called attention to suggestive exam
ples: 4 of lupus of the lobule of the ear following ear-piercing; 3 cases of
tuberculosis verrucosa cutis of the hands in laundresses who had washed
linen from tuberculous individuals; several cases of the same type, and
1 of lupus vulgaris, which apparently originated from tuberculous pa
tients in the same households. Elliot’s2 case of tuberculosis verrucosa
in a woman aged seventy is also an example of contagion; the disease,
which was on the back of the hands, developing after nursing and washing
the linen of a phthisical son. I have had as patients several young chil
dren with beginning face lupus, in families in which tuberculous indi
viduals lived and by whom they had been frequently nursed and caressed.
Ware3 reported an additional instance of tuberculous inoculation follow
ing ritual circumcision, and states that there is a record in literature of
21 such cases—and I believe probably even a greater number—as Dub-
reuilh4 collected 17 cases of tuberculosis of the penis consequent upon
this religious rite by consumptive operators. Ernst5 has collected 8
recorded cases (1 of his own) of cutaneous tuberculosis from tattooing.
That lupus and other cutaneous tuberculoses occasionally, although not
frequently, arise at the point of vaccination has been shown by Besnier6
and others, and quite recently another probable case came under Perry’s7
observation, and 1 also under Little’s8 notice, to which I can add 1 of my
own (the sister of a physician), the disease making its appearance
shortly after that procedure in early childhood, and when coming under
my care, ten or twelve years later, it had reached the size of a palm.
To this overwhelming evidence of the tuberculous character of these
various cutaneous processes and the communicability of the disease must
be added the success of experimental animal inoculation, notably by
Leloir,9 Eve,10 and Gougerot and Laroche,11 and the reactionary symp
toms brought about by tuberculin injections.
Pathology of Tuberculosis Cutis.—The tubercle bacillus,
being the accepted cause of the disease, its mode of entrance into the
cutaneous tissues other than by direct inoculation already referred to
remains to be solved. Sticker12 believes that in lupus, as well as in lep-
1 Wild, “Some Sources of Infection in Cutaneous Tuberculosis,” Brit. Med. Jour.,
Nov. 11, 1899, p. 1353.
2 Elliot, Jour. Amer. Med. Assoc, Jan. 12, 1889, also quotes statistics showing fre
quency of pulmonary tuberculosis in association with the cutaneous lesions.
3 Ware, New York Med. Jour., Feb. 26, 1898.
4 Dubreuilh and Auche, Archives de méd. exper. et d'anat. patholog., Sept., 1890, p.
601; abs. in Annales, 1891, p. 95 (in all, 60 collated cases of integumentary inoculation).
5 Ernst, Dermatolog. Centralbl., Dec, 1907, p. 66.
6 Besnier, “Lupus Vaccinal.” Annales, 1889, p. 576.
7 Perry, Brit. Jour. Derm., 1898, p. 196 (case demonstration).
8 Graham Little, ibid., 1900, p. 60 (case demonstration).
9 Leloir, Comp.-Rend. et Mémoire de la Soc. de Biol., 1882, p. 843.
10 Eve, Brit. Med. Jour. 1888, i, p. 644.
11 Gougerot and Laroche, Archiv de Méd. Exper. et d’ Anat. Path., Sept., 1908, No. 5,
p. 581; abs. in Brit. Jour. Derm., 1909, p. 125, claim to have produced lesions clinically
and histologically identical with several of the varieties of tuberculides that occur in
human beings; their method was not by inoculation, but to rub into an epilated surface
of guinea-pigs a virulent culture of tubercle bacillus.
12 Sticker, Dermatolog. Zeitschrift, 1898, vol. v, H. 6.
TLBERCULOSIS CUTIS
733
rosy, the primary lesion or infection is in the nose, and through the
lymphatics to the skin, and this, in face cases, which constitute the over
whelming majority of cases, seems, as also suggested by Leredde,1 Me-
neau and Frèche,2 and others, not improbable.3 Leloir4 believed the
bacillus gains access to the integument in one of the following ways:
(1) By direct inoculation from without; (2) indirect inoculation by con
tinuity from deep tuberculous foci; (3) inoculation by way of the lym
phatics or the veins passing through a tuberculous focus more or less
remote; (4) infection of hematic origin; (5) infection by inheritance; the
first two being probably, as I believe myself, the usual methods. Bes-
nier, quoted by Leloir, holds the view that the tuberculous ulcer of
phthisical patients is secondary to general infection, while lupus and
tuberculosis verrucosa cutis are the result of external inoculation.
It is doubtless probable that weakened tissue and regions disposed
to circulatory disturbance show less resistance to invasion. As in lupus
erythematosus, the “flushing” parts, as the cheeks, nose, ears, etc,
and dependent situations, where the circulation is sluggish, as the ex
tremities, and regions weakened by chilblains, are most vulnerable.
These are, it is true, the parts which are most exposed to injury and to
inoculation. Its tendency to appear primarily at the site of injuries
or in scar (weakened) tissue has also been noted, both by Crocker and
Malcolm Morris; in their treatises they refer to this, and an example has
been lately reported by Walsh,5 the disease making its appearance some
years after the scars had been produced. Hutchinson6 is disposed to
believe, in view of its frequently beginning after slight injuries, that a
stage of congestion and cell effusion, indistinguishable from common
inflammation, usually precedes for a short period the characteristic
growth. The arising of new points or foci beyond the main patch is
doubtless due, as suggested by this writer, to the bacilli or their products
spreading either in the perivascular spaces or along the lymphatic chan
nels. It is difficult, however, to explain the varying clinical conditions
1 Leredde (Hallopeau et Leredde, Traite pratique de Dermatologie, p. 468).
2 Meneau and Frèche, “Origine nasale du lupus de la face,” Annales, 1897, p. 516.
3 H. E. Jones, in an analysis, bearing upon this point, of 923 cases of lupus vulgaris
(Sequeira’s service, Skin and Light Department of London Hospital), Brit. Jour.
Derm., 1907, p. 305, was able to divide them into the following six groups: (1) 47.3 per
cent., arising as a small spot on face, cheek, or neck, including a few arising around the
margin of the eyelids and on the auricle, but not those springing from tuberculous
glands, or in scars of gland abscesses, or in scars left from the removal of old glands;
(2) 28.9 per cent., arising on the nose or in the nostril; (3) 11.4 per cent., arising sec
ondary to tuberculous glands, either in the scar or gland abscesses; (4) 1.8 per cent.,
arising from mucous membranes, other than the nasal, chiefly the margins of the lips;
(5) 1.8 per cent., arising secondary to tuberculous disease of the bones; (6) 8.5 per cent.,
arising in miscellaneous ways and on various parts of the body, and not, as far as
ascertained, secondary to tuberculous diseases of bone; also some, presumably a general
infection, in these cases, arising after the exanthemata or lowering illnesses, with mul
tiple lesions on various parts of the body. Philippson, in his recent valuable little book
on lupus (“Der Lupus, Seine Pathologie, Therapie, Prophylaxe, Julius Springer,” Ber
lin, 1911—translated from Italian MSS. by Juliusberg), states that in 135 cases the in
fection was primary in the skin in 42 cases, secondary to surgical tuberculosis in 53
cases, secondary to nasal tuberculosis in 26 cases, and hæmatogenous in 14 cases.
4 Leloir, Brit. Jour. Derm., 1894, p. 298.
5 Walsh, “A Case of Lupus in Symmetrical Seton Scars,” Brit. Jour. Derm., 1894,
P. 365.
6Hutchinson, Brit. Med. Jour., Jan. 7, 14, and 21, 1888.
734
NEW GROWTHS
found in cutaneous tuberculosis, but the individual nutrition, resisting
power, and possibly virulence of the bacillus may be of some importance.
A striking fact, however, is that in most instances there is but a single
type in the individual case, distinct and clean-cut throughout, only
occasional cases being observed in which several of the manifestations
are present in the same patient; and according to my own observations,
this latter seldom occurs so primarily.1 So distinctive are these types
usually that the possibility has often suggested itself that, after all,
we may be dealing with several varieties of bacillus, apparently mor
phologically and biologically the same, according to our present methods,
but which future investigations may lead to differentiation.
Leloir and Tavernier’s2 opinion as to the forms or certain phases of
lupus seems to me to offer a partial explanation of these cases—that
it is due to the combined action of the bacillus of Koch and suppurative
agents. They believe that there are two microbic processes—(1) neo-
plastic, due to the irritation of tubercle bacillus, and (2) suppurative,
due to the staphylococcus aureus, the latter, determining the presence
or absence of the ulcerative feature, not being found in the non-ulcerative
form. It is not improbable that the latter, and doubtless other infective
factors, added to an area of tuberculosis cutis in a subject in tropical
countries, may lead to destructive and persistent ulcerations, and furnish
some examples of the so-called “tropical ulcer.”
In lupus the bacilli are seen in extremely scant numbers, sometimes
scarcely to be found, in others not more than a single bacillus in a cell
(Cornil and Leloir). It is possible that the bacilli may undergo rapid
destruction, or that the morbid action results from their products or
toxins. It may be also, as Much’s investigations3 indicate, that there
may be other elements of tubercle organisms besides the ordinary bacil
lus, which so far have escaped the observation of investigators. In other
forms of cutaneous tuberculosis the bacilli are often found in greater
abundance, and this is especially so in the more acute lesions—as, for
instance, in the type described as tuberculosis ulcerosa.
The pathologic histology of cutaneous tuberculosis, more especially
lupus vulgaris, has been studied by numerous investigators (Virchow,
Auspitz, Lang, Kaposi, Friedländer, Thin, Jarisch, Leloir, Unna, Bowen,
and others), whose findings and interpretations in the main and essential
points coincide. Bowen,4 a careful and well-known dermatologist, has
given us an admirable and terse review and summary, based upon the
work of others and his own observations, and from which I shall largely
quote verbatim.
The disease has its starting-point in the corium, affecting primarily
1 Hoffman reports (Münchener Med. Wochenschr., 1909, No. 35) an interesting case
of associated types—multiple verrucous cutaneous tuberculosis with generalized “fol-
liclis” and transition forms.
2 Leloir and Tavernier, Jour. mal. cutan., Oct., 1891, p. 543.
3 The interesting investigations by Zieler, Much, Krüger, Friedländer and others
concerning the toxins and other forms of organisms (Much’s organisms), while not
conclusive, may tend to clear up some of the obscurity surrounding the etiology of the
tuberculides—see under “tuberculosis cutis” for brief notice and references.
4 Bowen, “The Pathology of Cutaneous Tuberculosis,” Boston Med. and Surg.
Jour., Nov. 12, 1891, p. 516; and Morrow’s System, vol. iii (Dermatology), p. 535.
TUBERCULOSIS CUTIS 735
the lower portions, progressing upward by extension of the foci of disease,
and causing, in most instances, secondary and non-specific alterations
of the epithelial elements. The first appearance of the lupus tissue is
found to be an accumulation of cells, situated about the capillaries and
lymph-channels, in many cases representing a growth of the adventitia
of these vessels, and constituting the primary nodule or point of infiltra
tion—of so-called granulation tissue—made up of the peculiar cell-
formations more or less characteristic of tuberculous processes: small
round cells, found abundantly at the periphery of the nodule; larger,
epithelioid cells, with clear nucleus, and the so-called giant-cells, with
homogeneous center and peripherally arranged nuclei. The epithelioid
cells are fewer in number, and the giant-cells in larger representation
than is observed in the classic tubercle of tuberculosis; there are, more
over, more vascularity and a greater formation of connective tissue.
Unna believes that many of the small round cells at the periphery of the
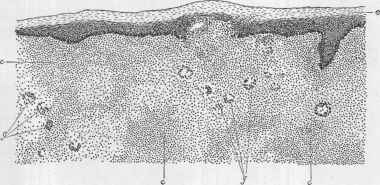
Fig. 168.—Lupus vulgaris section (low power): e, Epidermis; c, c, c, corium, infil
trated with the tuberculous neoplasm; g, g, Langhans’ giant-cells (courtesy of Dr. J. T.
Bowen).
lupus nodule are not leukocytes, but early derivatives of the connective-
tissue cells; he regards these as identical with the “plasma cells’’ of Wal-
deyer, and distinct from Ehrlich’s mast-cells. He has named these cells
plasma cells, and holds that they are the first appearances in various
chronic inflammatory and infectious processes. This view is not, how
ever, generally accepted. It would seem probable, as Bowen states,
that the fixed tissue-cells are, at least in the main, the parents of the
epithelioid and giant-cell formations. This giant-cell, when discovered
in lupus nodules by Friedländer, was, with cheesy degeneration of the
nodule, thought to be characteristic of tuberculous lesions, but it is now
known to be present in other pathologic processes, notably in the gum-
matous and small papular syphilitic lesions; still its presence, especially
when considered in connection with the other histologic features, and
with their formation and development, is of special significance. The
feature that is absolutely pathognomonic, however, is the bacillus, which
is constantly present, though sometimes sparingly.
736
NEW GROWTHS
The next stage in the history of the lupus nodule is the degeneration
of the newly formed cells and of the fibrillary tissue. The cells lying
in the center of the nodule are the first to be affected, their protoplasm
becomes homogeneous, while the nuclei lose to a certain extent their
susceptibility to staining. Following Weigert, the cells in lupus, as in
internal tuberculosis, are regarded as undergoing a coagulation necrosis,
although this view is opposed by Unna. At all events the tuberculous
elements undergo necrotic degeneration in consequence of the toxic
influence of the bacilli; owing to the small numbers of the latter it is
of slow progress. Together with this degeneration in the epithelioid
cells there is also a regenerative process—the cells are capable of prolifera-
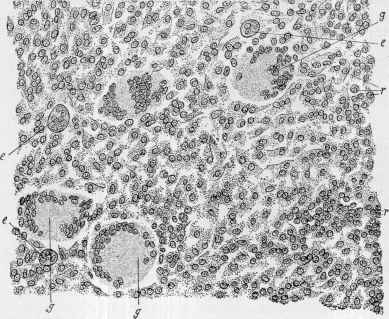
Fig. 169.—Lupus vulgaris section (high power): g, g, g, Langhans’ giant-cells; e, e, ey
epithelioid cells; r, r, small round cells (courtesy of Dr. J. T. Bowen).
tion when not affected by the virus to the extent of advanced degenera
tion, and may finally become converted into connective tissue. In this
manner is produced the lupoid scar tissue, which, however, Unna con
siders distinct from ordinary scar tissue; inasmuch as there is never a
reproduction of elastic fibers, the connective tissue is never arranged
in intersecting bundles, but placed horizontally to the surface, and it
contains numerous large “cell spindles” rich in protoplasm. If this
regenerative connective-tissue process is excessive, the hypertrophic or
elephantiasic feature of the disease sometimes observed results. Pro
liferation of the epithelial elements is also at times noted, which Bowen
considers an accidental and secondary process; the interpapillary down-
growths deep into the corium, with the outgrowth of the papillae, explain
TUBERCULOSIS CUTIS
737
the papillomatous forms. Lang also pointed out the occasional prolifera
tion of the glandular elements.
When the tuberculous infiltration of the corium reaches a certain
grade of intensity and the overlying epidermis is stretched and thinned,
a fracture of the latter frequently ensues, and the disease foci are exposed
and ulcerations result. In such instances, as noted by Leloir and Taver-
nier, there is probably, frequently at least, an added septic process, due
to the presence of pus-cocci.
In the lesions of tuberculosis ulcerosa (miliary tuberculosis of the
skin), as Bowen states, the cutis is found to be filled to a considerable
depth with foci of small round cells, with occasional epithelioid and giant-
cells. In the center of these foci the necrosis has progressed rapidly,
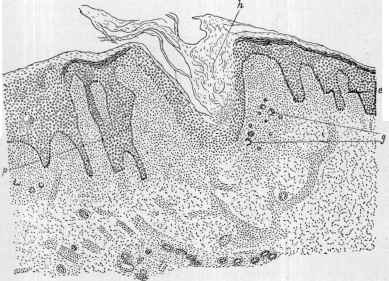
Fig. 170.—Tuberculosis verrucosa section: h, Hypertrophied horny layer, dipping
down into the corium; p, epithelial downgrowths, with enlarged papillae between them;
g, giant-cells; e, enlarged papillæ (courtesy of Dr. J. T. Bowen).
so that upon macroscopic examination the appearances of softening and
cheesy degeneration are apparent. The tubercles often, by their coali
tion, form masses of softened and necrotic tissue, in which the evidences
of unaltered granulation tissue can be found only in the outlying parts.
In the cases examined by Bowen the bacilli were present in large numbers,
in one instance every field containing enormous masses, according, as he
states, with the observations of Riehl, Doutrelepont, and others.
In scrofuloderma, according to Bowen, the anatomic characters
differ in no essential way from tuberculosis of the internal organs; granu
lation tissue of small round and epithelioid cells, with a moderate quan
tity of giant-cells, has its seat in the subcutaneous tissue, undergoes
degeneration, and may break through the thinned and tense layers of
the epidermis above, giving rise to the characteristic ulcer of this type.
47
738 NEW GROWTHS
The degeneration is, as a rule, much farther advanced than in lupus,
large areas of necrotic, softened tissue being usually visible under the
microscope. The bacilli in some instances are scanty, in others numer
ous, and generally much more so than in lupus, and in less abundance
than in tuberculosis ulcerosa.
In tuberculosis verrucosa the findings of Riehl, Paltauf, Bowen,
and others practically agree. Bowen states that the chief anatomic
characteristic of this form, in distinction from the papillary growths
of lupus, is the situation of the tuberculous neoplasm; while in the latter
the foci of granulation tissue lie in the lower and middle portions of the
corium, in tuberculosis verrucosa they are quite constantly found in the
upper papillary layers, usually in the papillæ themselves, and this cor
responds to the observations of Riehl and Paltauf. Moreover, the
papillary outgrowth is an early feature of the process, appearing at the
very beginning: in lupus, on the other hand, it is met with at a later
period, and, as a rule, only when ulceration has taken place. As Bowen
adds, many transitional forms occur, and it may be difficult, in some in
stances, from microscopic examinations alone, to determine which of
these two clinical varieties is represented. A characteristic of the typical
process, however, in most cases distinguishing it from other forms, is
the occurrence of foci of acute inflammation immediately below the rete,
and the formation of miliary abscesses, a secondary phenomenon due to
the invasion of micrococci; in some cases, however, Bowen has noted
this secondary inflammation to be very slight or entirely wanting.
Bacilli are found readily in some instances; in others a good deal of
careful search is necessary; and in this respect, while some observers
have noted the contrary, Bowen, in his examinations, was not able to
demonstrate a striking divergence from lupus.
Diagnosis of Tuberculosis Cutis—The diagnosis of the types
of tuberculosis cutis other than lupus vulgaris has been sufficiently
touched upon; these remarks, therefore, concern the latter, the form
with which practitioners are most likely to come in contact. The
peculiar yellowish-red infiltrated macule, point, or tubercle of soft con
sistence, readily disturbed by slight pressure with a probe or blunt
instrument, is an important characteristic of this type, and in itself
often sufficient for the diagnosis. The diseases of the skin with which
lupus vulgaris is sometimes confounded are epithelioma, more espe
cially of the superficial or rodent ulcer type, and syphilis; its confusion
with lupus erythematosus, acne rosacea, and eczema is much less prob
able. The difference between this disease and blastomycosis will be
referred to under the latter.
As to epithelioma, it differs from lupus in the following particulars:
it is usually single, begins commonly late in life, has a peculiar pearly,
roll-like, or markedly infiltrated border; it frequently arises from a pre-
existing mole or wart, or from a circumscribed, long-continued, scurfy
or crusted spot; the ulceration begins almost invariably at one point,
and is often somewhat deep, with frequently, and always sooner or later,
considerable loss of substance; its course in some cases is slow, but in
others, after the disease is once established, is frequently quite rapid.
TUBERCULOSIS CUTIS 739
The tubercular syphiloderm in many cases bears considerable re
semblance to lupus—in fact, these two diseases are often strikingly
similar in their symptomatology, and occasionally even the trained
specialist may for a time be puzzled.1 I find that with general prac
titioners the admitted respectability of a patient, especially if a woman,
is permitted to have too much weight, and leads often to an erroneous
diagnosis of lupus. It is not to be lost sight of, however, that syphilis
is often innocently contracted—as, for example, through the marital
relation. An important clinical fact bearing upon the diagnosis between
these two diseases is that lupus vulgaris is in this country comparatively
rare, and that the physician is much safer and almost always right in
considering a tubercular eruption with atrophic or ulcerative tendency
appearing in adult life to be syphilitic rather than that of lupus, unless
there are conclusive reasons for considering the contrary; and in a sur
prisingly large number appropriate treatment will confirm the tentative
diagnosis by the extremely rapid improvement which ensues. Generally
speaking, however, a careful study of the symptoms presenting will
render a purely arbitrary and unscientific method unnecessary, for in
almost all cases there are sufficient differences which will serve to prevent
mistakes. The common site of lupus is the face, and while it may appear
elsewhere independently, as a rule, when occurring upon other parts, it
is in conjunction with the disease upon the former region. The tuber
cular syphiloderm, on the other hand, occurs upon almost any part in
dependently, although it cannot be denied that the face is quite a fre
quent seat. This manifestation of syphilis being usually a late one, is,
for obvious reasons, more commonly observed toward middle or late
life; lupus, in most instances, has its start in childhood and early adoles
cence, and is somewhat rare in beginning after thirty or forty. The color
of the syphilitic eruption is a darker red, more of a coppery-red, while
that of lupus is more of a yellowish-red or brownish-red color. The
former is relatively more rapid in its course, and in a few years’ time may
cover several square inches, whereas in lupus several years often elapse
before more than a silver-dollar-sized area is covered. In syphilis cres-
centic and serpiginous groupings, crescentic and horseshoe-shaped
ulcerations are almost invariable: in lupus such conditions or configura
tion are uncommon. The ulcerations of syphilis may be superficial
or deep, those of lupus almost uniformly shallow; there is usually a
moderately or profusely abundant purulent discharge in the ulcerations
of the former, whereas in lupus destruction it is, as a rule, scanty—some
times extremely so. In the former disease bone may become involved
in the destructive process; in lupus such destructive action is rarely seen.
In lupus the cicatricial formation is often thick, dense, and tough,
whereas in syphilis it is usually soft and, when compared to the some
times preceding extensive ulceration, insignificant.
In the non-ulcerating forms of lupus and tubercular syphiloderm
the differentiation is often fraught with greater difficulty than in the
more common or ulcerating types. Most of the facts pointed out,
1 Stelwagon, “Remarks on the Destructive Skin Diseases: Epithelioma, Lupus
Vulgaris, and Syphilis,” Amer. Medicine, 1905, vol. ix, p. 643.
740
NEW GROWTHS
however, are also of service here. The history of the case is sometimes
valuable: in lupus not infrequently the patient comes of a tuberculous
family, with a history of consumption in the immediate or collateral
branches; sometimes an examination of the patient will disclose other
evidences of a scrofulous character, such as scars of a cervical adenitis,
marks of a keratitis, or even tuberculous involvement of the lungs. On
the other hand, in syphilis, upon careful inquiry or inspection, evidences
or history of preceding characteristic phenomena of that disease may
usually, but by no means always, be elicited. As already stated, how
ever, it must be admitted that in rare instances the several differences
mentioned as distinguishing these two cutaneous diseases are practically
lacking, or sufficiently so as to make a positive diagnosis without further
observation of the case almost impossible. Nor are the differences as
given absolute, as exceptions as to character, course, etc, are encountered
in both affections. In such instances, and, in fact, in all except those
cases in which the diagnosis can be made without difficulty and with
certainty, the general physician is much safer in withholding an opinion
or expressing himself guardedly, and in the meantime treating the patient
as if the disease were of syphilitic origin. When, in obscure cases, a
positive conclusion is urgent, resort may be had to the tuberculin and
Wassermann tests, but such would scarcely be necessary if a skilled
opinion was within reach.
Lupus vulgaris differs from lupus erythematosus chiefly in the pres
ence of papules, tubercles, and often ulceration and tough fibrous scarring,
all of which are wanting in this latter disease; moreover, the former is
lacking in the patulous or stuffed-up gland-ducts and the firm yellowish-
gray adherent scales, so commonly noted in lupus erythematosus. Lupus
vulgaris is almost always deeper seated. Lupus vulgaris erythematoides
of Leloir bears a close resemblance, but here also the deeper infiltra
tion and the lupus-infiltrated points or nodules which can generally be
recognized when the skin is put upon the stretch serve to distinguish it
from lupus erythematosus.
Acne rosacea merely exhibits an apparent similarity, but the dilated
vessels, acne lesions, and history and course, with absence of any tendency
to destructive action, are sufficient to prevent error. Both scaly eczema,
when rather sharply circumscribed, and psoriasis patches bear some like
ness to non-ulcerative or exfoliative lupus, but the infiltration of the
latter and its scant scaliness, its slow, sluggish course, and persistence
in the same spots will usually prevent all possibility of such a mistake.
Moreover, the itchiness of eczema and its occasionally frequently pre
senting a disposition to gummy exudation, and the more or less general
distribution of psoriasis, are further points.
In addition to the objective clinical characters, histologic features,
and history, the usual determining diagnostic factors in lupus vulgaris
and the other types of tuberculosis of the skin, in obscure cases recourse
may be had to a trial injection of tuberculin (combined systemic and
local reaction test), or to the so-called local reaction tuberculin tests,1
1 These are the ophthalmic (Calmette, Wolf-Eisner) instillation test, consisting of
the instillation of 1 drop of a ½ to 1 per cent, tuberculin solution in the eye, and the
TUBERCULOSIS CUTIS 741
and lastly, in extremely obscure cases, to experimental animal inocula
tion. A positive result with these tests is a fairly reliable indication
of the tuberculous character of the disease, but is not absolutely so.1
Fortunately, in almost all cases, a study of the local conditions alone will
usually be found sufficient to reach a positive diagnosis.
Prognosis of Tuberculosis Cutis.—As to the prognosis of
lupus vulgaris, much depends upon the age of the subject, duration
of the disease, extent of the territory involved, and the thorough co-
operation of the patient. It is always a chronic disease, usually ex
ceedingly rebellious to treatment, and one that calls for a guarded
opinion; moreover, relapses, sometimes due to inefficient or insufficiently
radical treatment, are not uncommon. According to my experience,
however, small beginning areas of the disease, especially in the young,
are usually readily curable, and, as a rule, show no tendency to relapse
if treatment has been sufficiently thorough. The same holds true with
small areas in the adult; and in areas of moderate size, more especially
in American born, permanent results are not unusual, although not infre
quently one or two relapses may occur before this favorable termination
is reached. In cases of considerable extent, if treatment is persisted in,
the final result is often satisfactory, even though outcroppings of tuber
cles in the scar tissue, or at the edge of the patch, as generally observed,
recur several times and call for further measures. One might feel hopeful
of more extensive cases if the patient’s continued co-operation were given,
but in many such instances the repeated disappointments experienced
from the recurrent evidences of the disease often lead to a total aban
donment of medical aid. It is true that in such cases the prognosis
must be guarded, for even with well-directed and persistent treatment
the malady is frequently rebellious and recurrent; and occasionally,
too, when the area involved is comparatively small, it is likewise noted
to be extremely obstinate. Fortunately, lupus does not thrive as well
von Pirquet, Ligniéres, and Moro tests. The von Pirquet test consists of scarifying
into the skin, as in vaccination, a drop or so of the tuberculin solution; the Ligniéres
test, rubbing in the solution on a closely shaved skin area; and the Moro test, rubbing
into a small area of thoroughly cleansed, thin and unbrcken skin 1 or 2 grains of a
tuberculin ointment, made up of equal parts of Koch’s old tuberculin and anhydrous
lanolin. If in the eye test a limited or general conjunctival redness or inflammatory
reaction of from mild to severe grade ensues in from a few hours to eight or ten hours,
abating in twenty-four to seventy-two hours, it is considered a positive indication;
this test should not be made if there is any disease of the eye or conjunctiva; the litera
ture contains some recorded accidents with it. On this account, in fact, the eye test
has been largely given up.
In the true skin tests (Ligniéres, Moro) a positive reaction, erythematous and papu
lar, in the area of application, following within thirty-six hours, and then disappearing
slowly in from five to ten days or so, is also considered strongly suggestive. (Trimble,
N. Y. Med. Jour., May 22, 1909, gives an account of some experimental trials with the
Moro inunction test, and Wilson, Jour. Amer. Med. Assoc, 1908, vol. 1i, p. 1836, gives
brief review (with references) and experimental trials of the eye instillation method.)
Kingsbury, Jour. Cutan. Dis., 1909, p. 78, reports favorable observations with the
latter method.
indeed, far from it if the observations by Augagneur (Thèse de Lyon, 1910, p.
103—abs. by Pernet, Brit. Jour. Derm., 1911, p. 87) are correct—that syphilitics, clin
ically non-tuberculous, react to the tuberculin tests in as great a percentage of cases
as tuberculous subjects. This seems to be corroborative of the earlier similar con
clusions reached by Nicolas, Favre, and Charlet that these tests did not seem to differ
entiate between syphilis and tuberculosis.
742
NEW GROWTHS
with us as elsewhere, and when it does occur, it is noted to be, as a rule,
less virulent and progressive, and generally yields much more readily
to therapeutic measures than is observed in those countries where the
disease is more common.
The danger of general infection is not to be forgotten, although in
most cases the health usually remains good and uninvolved; on the other
hand, death from tuberculosis of the lungs or general tuberculosis has
been, as already stated, noted in some instances, probably more fre
quently than is commonly believed. The statements under etiology as
to the frequency of the systemic tuberculous association are convincing
on this point, and to these may be added the observations of Besnier
and Leloir;1 the former noted that 21 per cent, of his lupus patients died
of consumption, and the latter refers to a number of instances in his own
experience in which pulmonary tuberculosis followed lupus through the
medium of the lymphatic system; Forchhammer’s record is likewise
startling.2
The prognosis as to the other forms of cutaneous tuberculosis has
been already incidentally touched upon. As a rule, they are, except
ing the disseminated type, more amenable to treatment, unless very
extensive. The same possibility, however, to general infection exists.
The prognosis of miliary tuberculosis of the skin is, as stated in its con
sideration, always grave.
Treatment of Tuberculosis Cutis.—While the remarks as to
treatment are more especially directed to that of lupus vulgaris, they
apply also to the other forms, modified, of course, to suit the different
conditions presenting. The most expedient methods for the latter have
been briefly referred to in connection with the description of these other
varieties.
The rational management of lupus keeps in view the supervision of
the patient’s general health, together with the employment of local
measures having as an object destruction or removal of the diseased
tissue. As a rule, but little stress is placed by most writers upon con
stitutional treatment, but in accepting the tubercle bacillus as the essen
tial factor of the disease, with the frequent association of allied and
systemic tuberculous affections observed, the importance of general
measures (not necessarily medicinal) cannot, in my judgment, be ignored
if the best results are to be attained. In short, the patient, as well as
his cutaneous disease, must receive attention: good, nutritious food,
fresh air, outdoor exercise, and plenty of sunshine, with, in many cases,
the administration of such remedies as cod-liver oil, hypophosphites,
iron, quinin, and other alterative tonics. Judged by my own experi
ence, cod-liver oil in small or moderate doses long continued is the most
valuable of the internal remedies, and has in some cases a material in
fluence in limiting the spreading or active tendency of the disease, and
1 Besnier, “Le lupus et son traitement,” Annales, 1883, p. 377; Leloir, “Les rapports
du lupus avec tuberculose,” ibid., 1886, p. 328.
2 Forchhammer, Archiv, 1908, vol. xcii, p. 3 (with review of subject), states that of
1190 lupus patients treated at the Finsen Institute during ten years, whose history
could be followed, 143 had died, and of these 81 died of tuberculous diseases; 58 of these
of tuberculosis of the lungs.
TUBERCULOSIS CUTIS 743
in aiding toward making the results from local treatment more perma
nently favorable; in other words, rendering the soil a less favorable hab
itat for the bacillus. The hypophosphites have also proved of service.
Other remedies have likewise been credited with favorable effect.
The syrup of the iodid of iron is one which has had some support,
and Liveing commended 3 to 5 minims (0.18-0.3) of tincture of iodin,
sometimes associated with a few drops of Fowler’s solution. Duhring1
believes that potassium iodid favorably influences some cases, and also
speaks well of iodin and phosphorus, in combination with cod-liver oil.
Lately Philippson2 stated that the internal use of parafluorbenzoate of
sodium, in 7- or 8-grain doses (0.465-0.533) three times daily, acts
favorably; and Stepp3 commends fluoroform (CHF13), a gaseous sub
stance taken up by water to the extent of 2.8 of its volume, and of this
solution the dose is 1 to 4 drams (4.-16.), four or five times daily. Sev
eral observers—Bramwell and Taylor4 and a few others—have seen a
favorable influence exerted by thyroid feeding or thyroidin. Taylor
does not consider it safe for outpatients, inasmuch as to obtain satis
factory influence acute thyroidism must be produced; and he further
adds that it is only likely to benefit those in which there is much chronic
inflammation marking the disease, or where ulceration is taking place.
According to Pringle,5 in cases of lupus in which the hyperemic or in
flammatory element is marked, thyroid feeding had given results little
short of marvelous in many instances under his observation and without
necessarily producing the disagreeable phenomena of thyroidism.
Tuberculin injections, which at one time aroused the hopes of the
dermatologic world, have been, undeservedly I believe, almost wholly
abandoned, but a careful review of the earlier experiences and recent
observations with the new tuberculin show the remedy to be of distinct
value in many cases, although its use requires caution and care. Many
of the earlier experiments proved, upon the whole, of distinct benefit,
but the unfavorable reports of its trial, more especially in St. Louis
Hospital, Paris, by Besnier and Hallopeau,6 and the deaths reported as
following its use in lupus,—1 by Hallopeau and 1 each by Jarisch, Burck-
hardt, and Blanc,7—brought it rapidly into disrepute. In the past few
years, however, there has been a slight rebound, the new tuberculin
being employed, and apparently without injurious results, and with
alleged favorable influence upon the disease (Bukovsky, Napp and
Grouven, Krzysztalowicz, Ravogli, G. H. Fox, Lustgarten, Wright, and
others).8 An impartial judgment of the facts at hand would seem to me
1 Duhring, Diseases of the Skin, third edit., 1882, p. 481.
2 Philippson, Dermatolog. Zeitschr., 1899, No. 3.
3 Stepp, abs. in Monatshefte, 1899, vol. xxix, p. 551.
4 Bramwell, Brit: Jour. Derm., 1894, p. 345; Stopford Taylor, ibid., p. 345.
5 Pringle, ibid., 1899, p. 433.
6 Full abs. in Brocq’s Paris letter, Jour. Cutan. Dis., 1891, p. 191.
7 These 3 cases are cited by Piffard (with brief abstracts and references), ibid.,
1891,p. 172.
8 It has recently been tried by the following observers, and in the number and vari
ety of cases stated, usually with favorable, but variable, influence: Bukovsky (Jan-
ovsky’s clinic), Archiv, 1898, vol. xlvi, p. 223 (15 cases lupus, 2 of scrofuloderm, and
2 of tuberculosa verrucosa cutis); Napp and Grouven (Doutrelepont’s clinic), ibid.,
p. 399, with bibliography (39 cases, of which 36 were of lupus, 2 tuberculosis cutis,
744 NEW GROWTHS
to justify, in recurrent cases which had proved rebellious to other means,
the use of the new tuberculin (tuberculin R.—TR.), not with the belief
of its being curative in itself, but as a substantial aid in rendering the
local measures more effectual. Most observers, among whom those above
named, who have largely employed it, do not claim that it cures, but
accord it value as an adjuvant. The first dose should be small and subse
quent dosage and frequency regulated by its action or by the opsonic
index (Wright) of the blood; overdosage and too great frequency, it is
to be noted, would lessen the opsonic power, or phagocytosis, and
probably do damage, and are therefore to be guarded against.1
Injections of thiosinamin have been recommended by Hebra, Jr.,
using a 15 per cent, alcoholic solution, of which the beginning dose is
about Miv (0.265) increasing to Mxv (1.); an injection is administered
every two or three days. As with tuberculin, it is to be looked upon
as an adjuvant only, and should be combined with suitable local meas
ures. Calomel injections have also recently had some support as aux
iliary treatment of value (Asselbergs, Du Castel, Brousse, and Tschle-
now),2 an injection of about f of a grain (0.05) in 1 cc of sterilized oil
being administered, usually in the buttocks, every week or ten days.
Fournier3 is inclined to consider such cases of syphilitic nature, and that
the favorable effect are explainable upon an error of diagnosis.
Local Treatment.—The Finsen method and the x-ray are playing
an important part in certain centers in the local treatment of this disease,
but these are, for various reasons, often inconvenient or impracticable,
and, before referring to them specifically, the plans long in vogue and still
quite generally employed will be described. These measures can be
roughly divided into: (1) mild and stimulating; (2) destructive. In
almost all cases the area of apparent disease can be materially reduced
1 tuberculosis of tongue; in 2, serious symptoms of collapse without recognizable
reason); Krzysztalowicz, Wien. med. Wochenschr., 1898, pp. 59 and 108 (13 cases);
G. H. Fox, Jour. Cutan. Dis., May, 1898, p. 232; Lustgarten, ibid.: Bussenius and Coss-
mann, Das Tuberkulin R.—seine Wirkung und seine Stellung in der Therapie der inneren
und äusseren Tuberkidose, Hirschwald, Berlin, 1898; Adrian, Archiv, 1898, vol. xlv, H.
1 (in one of his cases, lupus of the face complicated with chronic nephritis, dangerous
symptoms arose); Van Hoorn, Deutsche med. Wochenschr., 1898, No. 27 (greatest
improvement between the first dose and maximum dose (20 mg.)—above that failed to
influence and sometimes was damaging); Porges, Wien. klin. Wochenschr., 1898, p. 366
(improvement at first); Heron, Brit. Med. Jour., July 9, 1898 (refers to 5 successful
cases with old tuberculin, and 1 case with new tuberculin); Starck, München. med.
Wochenschr., April 26, 1898 (3 cases—2 cured, 1 unfavorable); Taylor, Brit. Med. Jour.,
July 9, 1898 (first weeks improvement, later stationary, and then a recrudescence);
Ravogli (“Tuberculin in Dermatology”), Chicago Clinic, 1897, p. 143 (favorable influ
ence; with brief review of the subject and some references). See also recent interesting
paper by McCall Anderson, “A Plea for the More General Use of Tuberculin by the
Profession,” Brit. Jour. Derm., 1905, p. 317 (with illustrations), and same paper in
French in Revue pratique, 1906, p. 175; R. C. Low, “Tuberculin in Diagnosis and Treat
ment,” Scottish Med. and Surg. Jour., May, 1905, and in French in Revue pratique,
1906, p. 100.
1 For further remarks on this method and literature references, see “Opsonins,”
p. 108.
2 Asselbergs, Annales, 1898, p. 10 (25 cases; in some cases slight amelioration only,
in others marked improvement, and in others complete disappearance); Du Castel, ibid.,
1898, p. 674, and 1899, p. 527 (3 cases; 2 cases improvement, 1 uninfluenced); Brousse,
Jour. mal. cutan., April, 1899, p. 235 (1 case; favorable effect); Tschlenow, abs.-ref.
in Monatshefte, 1899, vol. xxix, p. 549 (2 cases; favorably influenced).
3 Fournier (“Pseudo-lupus syphilitique”), Annales, 1896, p. 854.
TUBERCULOSIS CUTIS 745
by the former, partly by controlling the inflammatory element of the
malady, and in some by a possible effect upon the bacilli and their prod
ucts or upon the added pyogenic organisms. The mildly antiseptic
plans are, especially in the crusted and ulcerative forms, in accord with
the well-based views of Leloir and Tavernier,1 referred to. Leloir was,
therefore, accustomed to direct his whole treatment primarily against
the staphylococcus aureus as a preliminary to a final more active plan
against the neoplastic growth due to the bacillus. If the disease is at all
extensive or attended with destructive changes, the use primarily of the
mild or nondestructive applications is to be advised. When the
hyperemic element is pronounced and there is any irritability, the fre
quent or constant application of the calamin-zinc-oxid lotion can often
be used temporarily with considerable apparent benefit. The continu
ous application of a good diachylon ointment is also found valuable at
this time. One of the best of the milder preparations, however, is an
ointment of oleate of mercury, which, in a few instances, proved useful
in my hands.2 Brooke’s3 formula is the most satisfactory: R. Oleate of
mercury, 5 per cent., 3j (32.); powdered zinc oxid and powdered starch,
ää 3ij (8.); white vaselin, 3iv (16.); salicylic acid, gr. xx (1.35); ichthyol,
Mxx (1.35). This can be colored the skin tint by adding 10 to 30 grains
(0.65-2.) of calamin or some Armenian bole. If the surface of the in
volved area is unbroken, this is to be rubbed in for several minutes
night and morning, and, when possible, also spread upon lint and kept
continuously applied as a plaster; if ulcerated, the latter method is the
only feasible one. The constant application of mercurial plaster is also
of value in many cases. It is possible the mercurial preparation has a
bactericidal action, as Doutrelepont,4 and later White,5 had already,
from clinical results, pointed out in their use of corrosive sublimate
applications. White employed lotions of 1 to 2 grains (0.065-0.13 5) to
the ounce (32.), and an ointment of the same strength; the former he
found more satisfactory in the tubercular and all closed forms, and the
latter on open ulcerated and crusted surfaces. The application is to be
made twice daily. Other remedies of allied action to that of the mercu
rials are sulphurous acid, advised by Hutchinson;6 salicylic acid (salicylic
acid, 3j-iss (4.-6.); vaselin, 3j (32.)), or 2 to 10 per cent, strength, as
recommended by Marshall;7 guaiacol, as recently extolled by Funk
and Alivisatos,8 with occasional applications of a 10 per cent, lactic acid
solution. Sulphurous acid is also esteemed by Harrison.9 Guaiacol
was variously used—pure, with equal parts glycerin or with equal parts
1Leloir and Tavernier, loc. cit.
2 Stelwagon (Clinical Lecture on Lupus, with illustrations), International Clinics,
July, 1896, p. 341.
3 Brooke, “A Preliminary Treatment of Lupus Vulgaris,” Brit. Jour. Derm., 1890,
p. 145; “On the Treatment of Scrofuloderma and Lupus,” ibid., 1891, p. 383.
4 Doutrelepont, Monatshefte, 1884, p. 1.
5 J. C. White (“On the Treatment of Lupus by Parasiticides”), Boston Med. and
Surg. Jour., Oct. 25, 1885.
6 Hutchinson, Med. Times and Gazette, April 26,1884.
7 Marshall, Brit. Med. Jour., June 25, 1884, p. 1253.
8 Funk, Monatshefte, 1899, vol. xxix, p. 216; Aliyisatos, La semaine médicale, 1900,
p. 10 (guaiacol and olive oil, each, 4 parts; alcohol (60 per cent.), 1 part).
9 Harrison, Brit. Med. Jour., Aug. 6, 1892.
746
NEW GROWTHS
sterilized olive oil, and applied frequently; and with, occasionally, other
more active measures. The compound lotion of zinc sulphate and potas
sium sulphuret advised in acne and lupus erythematosus is also often
useful as a preliminary application. Iodoform, usually as an ointment,’
5 to 15 per cent, strength, has had some praise, but it is not superior to
other remedies already mentioned, and which are free from the all-per
vading odor of this drug. The mild preparations, which, however, have
been most employed by myself, are the calamin-zinc-oxid lotion and
the oleate of mercury ointment, generally as in the formula prescribed
by Brooke.
One soon finds, however, in the great majority of instances, that
if much advance is to be made, recourse to stronger remedies is neces
sary; and if the area of disease is small, and in cases in which time is. a
consideration, it is best to adopt such measures from the start. First,
as to those of moderate activity, which are not usually actively destruct
ive. The best of these are salicylic acid, resorcin, and pyrogallic acid.
The first—salicylic acid—may be prescribed in several ways—in collo
dion, 30 to 60 grains (2.-4.) to the ounce (32.); in plaster mass, made
up with petrolatum and resin plaster, 1 to 2 drams (4.-8.) to the ounce
(32.); mixed with sufficient glycerin to make a paste, as recommended
by Treves; and as Unna’s plaster-mull. This last is made in several
strengths; the weakest can be placed among the mild remedies already
mentioned, the strongest, which are here referred to, containing respect
ively about 1 ounce (32.) and 1½ ounces (50.) to the spread meter, and
with about the same quantity of creasote, which lessens the pain of the
application. Unna,1 Jamieson, and others have warmly commended this
plaster-mull, more especially in the superficial and non-ulcerative types,
and from its use in several cases I can subscribe to its value. It is kept
continuously applied, changing daily; the tubercles undergo destruc
tion, and are, so to speak, shelled out. A 10 to 20 per cent, salicylated
collodion is also satisfactory. In ointment form, used 2 or 3 drams
(8.-12.) to the ounce (32.), and kept constantly in contact, it is also quite
active. I have had no experience with the salicylic acid glycerin paste.
Resorcin can be employed in the same manner and strength as salicylic
acid, most commonly as a strong ointment. As a rule, it is not
painful.
Of the several remedies just named, however, pyrogallol, originally
recommended by Jarisch, is in my experience the most certain in action.
Upon the whole, it is best employed as a stiff ointment, made up with
resin cerate and vaselin, or with some resin plaster added during the warm
season. I have not had much success, however, with the 10 per cent,
strength as commonly advised, nor secured action in several days, as
Jarisch and others reported; on the contrary, I can agree with G. H.
Fox2 that to secure effective result a strength of at least 25 per cent,
should be employed, generally in about one-third proportion. During
1Unna, Aerztliches Vereinsblatt für Deutschland, No. 166, 1886; Lancet, Sept. 25,
1886.
2 G. H. Fox, “The Therapeutics of Cutaneous Tuberculosis,” Boston Med. and
Surg. Jour., Nov. 12, 1891.
TUBERCULOSIS CUTIS
747
the cooler season an ointment made up as follows can be used: R. Pyro-
gallol, 3ij-iij (8.-12.); vaselin and resin cerate, ää q. s. ad 3j (32.).
This is spread thickly upon patent lint or any other suitable material,
and kept closely applied, changing to a fresh plaster twice daily. At
each renewal the parts are wiped off gently with a piece of soft linen or
cotton, and any loose skin, crust, scale, or slough thus removed. At the
end of five to eight days it is usually noted that a superficial slough or a
slough of variable thickness has formed, which may be more or less ad
herent. This, if but slightly adherent, may be rubbed off or picked off;
if firmly adherent,—and this is more commonly the case,—poultices are
to be applied until it softens and comes away, which may require several
hours or a day or more. The parts are then gently washed with soap and
water, rinsed, and wiped dry, and the pyrogallol ointment reapplied;
and so on until the destructive action has been deemed sufficient. A
course of such treatment usually requires from ten days to two or three
weeks. After removing the final slough a carbolized resin cerate or an
ointment of pyrogallol of 1 or 2 per cent, strength may be used, and
healing allowed to take place. Others follow this treatment, as I have
also done in some instances, with an ointment made up of equal parts of
mercurial plaster and petrolatum or with pure mercurial plaster. After
thorough healing it is often seen that in places the disease is still persist
ent, or soon afterward new foci reappear in the scarred tissue; the same
method is to be resumed, usually for a shorter period.
Belonging in this same class, or occupying a middle position between
these and the more destructive caustics, is arsenic, in the form of an
ointment or paste. It is one of the older methods, but, in my opinion,
is far superior and more effectual than many of the newer remedies. For
application to areas of 2 or 3 square inches to that of a palm an oint
ment used by Hebra, consisting of arsenious acid, gr. xx (1.35); cinnabar,
3j (4.); cold cream, 3j (32.), is to be commended. In order to diminish
the pain of the application—its greatest drawback—5 to 10 grains
(0.35-0.65) of cocain muriate can be added. This is spread, somewhat
thickly, upon lint and covered with wax tissue and bound on; it is changed
twice daily, and continued from two to four days. Considerable edema
and inflammatory swelling result, which, however, soon subside after
the arsenical application has been discontinued. Its action is, unless
too long continued, only on the diseased tissue; the nodules and other
lupus infiltration are converted into a grayish, necrotic mass. The
after-treatment for several days should, when possible, consist of poul
ticing until the sloughs come away, and then subsequently a 1 or 2 per
cent, pyrogallol salve, or an ointment of equal parts of mercurial
plaster and vaselin. As with all other methods, the arsenical applica
tion may have to be repeated one or more times before a permanent
result is reached. If the area of disease is quite small, the arsenical
application can be made in the form of a strong paste with acacia, as
advised in epithelioma.
Among other remedies of this same class may be mentioned lactic
acid, strongly commended by Mosetig. It is chiefly prescribed in the
ulcerative types, and applied on a wad of cotton for ten to thirty minutes,
748 NEW GROWTHS
once or twice daily at first, and during the interim using a mild salve,
such as boric acid ointment or a 5 to 10 per cent, aristol ointment.
Various caustics, in addition to the safer preparations mentioned,
have been advocated from time to time, such as Vienna paste, fuming
nitric acid, chlorid of zinc (see Epithelioma), but these are rarely resorted
to at the present day. The galvanocautery, however, has been strongly
urged by Besnier1 and others, using variously shaped knives and points,
practically combining cauterization with scarification. The Paquelin
cautery has also been variously advocated, and Unna often employs this
in conjunction with the plaster-mulls. Somewhat similar is the Höl-
Fig. 171.—Galvanocautery needle, knife, and spiral points (Besnier).
lander hot-air treatment, or hot-air cauterization2 by means of a suitable
apparatus, by which air heated up to several hundred degrees is projected
on the surface. It requires anesthesia and some skill and care not to
go beyond the safety limit. Properly managed, however, according to
reports, its effects are excellent. Plonski3 saw 1 case practically cured
in one sitting. Like all heat-cautery methods, however, it is potent for
evil if poorly handled.
Liquid air and carbon-dioxid snow (q. v.) have both been tried in
a few instances in lupus vulgaris for their cauterant action. They are
less violent and less destructive, but more manageable, than thermo-
caustics, and may have a field of usefulness in superficial areas of disease.
Fig. 172.—Multiple scarifier (as modified by Van Harlingen).
Of the operative methods which have been practised from time to
time, is to be especially mentioned that by curetting. Volkmann
originally suggested it, and since then it has figured largely in the treat
ment of this disease. It can be employed when patients do not object
to operative measures, in conjunction with caustic applications; and the
two together constitute a plan of treatment to be warmly commended.
1 Besnier, “Le lupus et son traitement,” Annales, 1880, p. 687, and 1883, p. 377 (a
review of the various methods, and especially descriptive (1883) of his own favorite
method, with cuts of instruments).
2 Hollander, Deutsche med. Wochenschr., 1897, p. 688; Berlin, klin. Wochenschr.,
July 12, 1899.
3 Plonski, Monatshefte, 1899, vol. xxix, p. 562 (case demonstration).
TUBERCULOSIS CUTIS 749
Etherization is usually necessary. The parts are thoroughly curetted,
the edges being well looked after. Inasmuch as some morbid cells or
tissue are left, a supplementary cauterization is an essential part of this
method. One of two plans can be used: either momentary cauteriza
tion with caustic potash in stick or strong solution, or several days’
use of a 25 per cent, pyrogallol salve. The latter, I believe, assures less
chance of recurrence. The subsequent treatment is the same as follow
ing the caustic methods. Linear scarification, warmly advocated by
Vidal, and which had the strong support of Morrow, Brocq, Squire,
Malcolm Morris, Stopford Taylor, and others,1 has practically given place
to other methods.
Excision has from time to time had support, but rarely employed
until Lang2 gave it the weight of his advocacy, although Clark,3 Bid-
well,4 and a few others5 previously or since have reported favorable
results. It has not been looked upon with favor in England or this
country, except for circumscribed areas. The method consists in com
plete excision, going well beyond the borders of the disease, and then
supplementing with Thiersch grafts usually immediately after the opera
tion. Lang’s great success with this method, which he now combines
1 Morrow, “The Mechanico-surgical Treatment of Skin Diseases,” Jour. Cutan.
Dis., 1888, p. 132; Stopford Taylor, “A Comparison of the Various Methods of Treat
ing Lupus Vulgaris During the Past Twenty Years,” Brit. Jour. Derm., 1894, p. 345.
Both papers give reviews of the subject and more or less details of the principal methods
in vogue. Brocq, Paris letter, Jour. Cutan. Dis., 1888, p. 103, gives Vidal’s method of
quadrilateral linear scarification in minute detail.
The method of procedure in linear scarification is as follows: the parts are thoroughly
gone over with close parallel incisions, 1/8 to 1/6 inch part, reaching down through the dis
eased tissue, and then the area is cross tracked in the same manner. Taylor finds it
unnecessary, as a rule, to cross-track the incisions, as in so doing the epidermis is likely
to be torn off, the papillæ exposed, and suppuration ensue, healing being thus delayed.
The hemorrhage is rarely troublesome, and is, as a rule, readily controlled by a wad of
cotton. There, is no question about the excellent cosmetic effect of this method, and
in nose cases, where there has been a good deal of destructive deformity, it saves tissue
and even seems to create new tissue, so that the deformity is much diminished. On
operating on the nose the nares are firmly supported by plugging with cotton or lint,
so as to have a good foundation. The objection raised against the operation by Unna
and others—that it makes auto-infection possible—is not supported by the observa
tions of those who have most frequently performed it. Multiple puncture (Dubini,
Volkmann, Veiel) is a somewhat similar operation, with which Volkmann was accus
tomed to supplement erosion with the curet, and it has been employed independently,
but is less satisfactory than linear scarification.
2 E. Lang, “Der Lupus und dessen operative Behandlung,” Vienna, 1898; also
(later communication on the results, with illustrations) Wien. med. Wochenschr., No.
38. 1900, and (later paper) Deutsche Med. Wochenschr., Oct. 7, 1909. Lang’s experience
has been large—412 cases since 1892; in 262 cases out of 291 reëxamined, at least six
months after the conclusion of treatment, good results still remained. He now com
bines excision and the Finsen method; und Deutsche Med. Wochenschr., June 23,1910.
In this number of the Wochenschrift other methods of treatment are also reviewed:
Finsen treatment by Zinsser, Radium treatment by Wichmann, and other methods
by Gottschalk.
3 Bruce Clark, Lancet, Mar. 18, 1893 (7 cases).
4 Bidwell, Brit. Jour. Derm., 1893, p. 288 (4 cases—1 relapse).
5M. B. Hutchins (2 cases), Jour. Amer. Med. Assoc, Dec 12, 1896, p. 1223;
Popper, Dermatolog. Zeitschrift, 1897, vol. iv, H. 1 (Lang’s method—34 cases, only 3
recurrences; gives minute details of cases and operation); Buschke, Archiv, 1899, vol.
xlvii, p. 23 (18 cases); Urban, Monatshefte, 1898, vol. xxvi, p. 429; Tavastsjerna, abs,-
ref. in Jour. Cutan. Dis., 1899, p. 148 (18 cases—a large number involving nose and
mouth; cure held in 5 cases two years after operation); Nélaton’s, Jour. mal. cutan.,
Jan., 1900.
750
NEW GROWTHS
with the Finsen treatment, is well worthy of more general adoption.
The chief objection is the disfigurement.
For destroying lupus tubercles which are isolated, more especially
those that spring up in the scar tissue, and often irrespective of what
the active plan of treatment has been, a sort of a double burr (Mal
colm Morris) or ordinary dental burr (G. H. Fox)1 has been warmly
commended. For the same purpose, as well as for the systematic treat
ment of cases, the pointed silver nitrate stick has been used, particularly
in Vienna; it is easily bored into the discrete tubercles, and while it thus
disturbs and destroys the body of the lesion, its mild cauterizing action
is damaging to the morbid cells with which it comes in contact. It is
rarely resorted to today, scooping out with the curet, the burr, or the
electric needle being far preferable if an operative method is elected.
Electrolysis may likewise be used for circumscribed patches, in a
manner originally proposed by Gartner and Lustgarten2 and since com
mended by Jackson.3 The former used a silver metal plate, and the
latter one of zinc, with a rim of hard rubber projecting about a milli
meter beyond the metal, to protect the healthy skin or to prevent too
severe action at the edge, the diameter of the plate being from ½ to 4/5
inch; this is attached to the negative pole, the anode sponge elec
trode being placed at any convenient point. The current strength
required is from 5 to 10 milliampères. The plate electrode is pressed
gently upon the patch to be treated, and the current passed for about
seven or eight minutes. The area is gone over at intervals of a week
for a few times, and then the isolated tubercles which are left are treated
with the electric needle, using a current of 3 milliampères. In this
same class of cases liquid air or carbon-dioxid snow can be used as a
cauterant.
(Two other methods of increasing importance, and which in coun
tries or centers where lupus is more common have to some extent sup
planted the plans of treatment formerly in use, are the Finsen-light
treatment and the Röntgen-ray treatment.)
First as to the Finsen treatment.4 Finsen and his capable assist
ants, Bang and Forchhammer, have been practising the method devised
by him, at his institute at Copenhagen, for some years, and with final
results eminently satisfactory. As referred to in the introductory
chapter the method is thought to hinge upon the bactericidal properties
of concentrated chemical rays, using the arc light, and controlling or
preventing the action of the heat rays. Others, among whom Lereddle,
Sequeira, Malcolm Morris, Hyde and Montgomery, and Lesser, have
also reported favorable results, so that the method is now regarded as
one of the most important in the therapeutics of this disease.
During a visit to Copenhagen, some years ago, I had the pleasure
of observing this method as practised by Finsen himself. The favorable
1 G. H. Fox, “On Various Methods of Treating Lupus Vulgaris, Including the Use
of Burr and Hook,” Jour. Cutan. Dis., 1885, p. 70.
2 Gartner and Lustgarten, Wien. med. Presse, 1886, p. 776.
3 G. T. Jackson, Jour. Cutan. Dis., 1890, p. 416.
4 See under General Remarks on Treatment regarding apparatus and other points
not here considered.
TUBERCULOSIS CUTIS
751
results and the excellent cosmetic effects were well in evidence.1 I am
not able to escape the conviction however, that, with some of the other
methods mentioned, as thoroughly and persistently carried out, the same
end could be attained, but probably with not as good cosmetic results.
Where lupus is at all common—or, say, not rare or uncommon, as it is
with us—the Finsen-light treatment can be efficiently and easily con
ducted, owing to proper training of the attendants in the’ technic.
On the other hand, where only an occasional case of the disease is met
with, it will, owing to the lack of proper training in its application,
scarcely supplant the other known methods—unless there are still
further improvements in the apparatus and a considerable shortening
of the time of exposure.
The duration of an exposure with the Finsen or Finsen-Reyn lamp
varies from three-quarters to one-and-a-half hours, depending upon
whether the disease is superficial or deep. It is usually necessary to
repeat the treatment on the same area at least once or twice, but before
a new exposure is made the reaction from the preceding one should have
been allowed to subside; this ordinarily requires, on an average, about
ten days. The reaction comes on from a few hours to a day after the
exposure, and varies from an erythematous to a vesico-bullous character;
there is no necrosis. When the disease is extensive, one area after
another can be treated, so that it often is necessary to give a daily séance,
and then several months, or much longer, may be required before the
entire involved surface has been sufficiently covered. Patients should
report a few months after an apparent cure for examination, and the
exposures resumed should there be any evidence of lupus tubercles or
infiltration. For superficial types, the first part of the treatment can
be done with the lamp of the Lortet and Genoud model, or with the iron-
electrode lamp; this will often act satisfactorily and relatively more
rapidly in removing a great part of the disease, and then the Finsen or
Finsen-Reyn lamp can be subsequently used for the remaining deeper
lupus deposits. The same combined plan can in many cases be satis
factorily adopted with the Röntgen-ray and Finsen treatments; the for
mer being employed first, and when the disease area has been reduced
to one or several obstinate patches the Finsen treatment can be resorted
to. In Copenhagen, in some instances, in order to shorten the period
of treatment, there is a preliminary treatment of the deeper-seated areas
with pyrogallol applications, as already outlined. In ulcerated areas, a
preliminary treatment by any appropriate plan is necessary before the
Finsen treatment is resorted to, as this cannot be used satisfactorily upon
ulcerated surfaces. Its special field is in the dry non-ulcerative cases.
When the mucous membranes, as in the nose, etc., are affected, the
1 Forchhammer, Finsen’s able associate and successor (abs. in Brit. Jour. Derm.,
1911, p. 338) reports that in the fifteen years of its use at Finsen Institute 2000 patients
had been under treatment, 1200 of whom had been followed up:—cured 721, or 60
per cent.; under treatment 217, or 18 per cent.; treatment discontinued 131, or 11 per
cent.; dead 131 or 11 per cent. More than one-half of the cured patients have been
free from recurrences for from two to ten years. About 80 per cent, of the “initial”
(somewhat recent and more or less limited) cases are cured; and about 50 per cent, of
the inveterate cases (extensive and of long duration).
752
NEW GROWTHS
disease cannot be satisfactorily treated with the light. Such regions
are to be handled as described later.
The favorable reports of the curative action of the x-rays1 in lupus
made by the pioneers in this method (Schiff, Freund, Neisser, Pusey,
Kummel, and others) have been corroborated by many other observers,
and it has now become, along with the Finsen plan, one of the accepted
methods. I can fully endorse its great value in some cases. One cannot
say, however, in a given case how much good it will do, and in some
instances it seems to have but little influence; in others, only after con
siderable reaction has been produced; and in others again, not till the
danger-point of Röntgen-ray reaction has been passed. Nevertheless,
it shares the honors at present with the Finsen light, and to some extent
has supplanted it. Its great advantage is that a large part or the entire
diseased surface can be treated at the one time, and in cases which show
response to its influence a good result is comparatively quickly obtained.
In a few instances a favorable action is noted without the production of
x-ray erythema, but ordinarily it is necessary, for the best and most
rapid effect, to bring about a moderate and continuous reaction; some
times it is necessary to push it to the point of x-ray dermatitis of the
second degree—vesiculation or serous exudation—before an impression
is made upon the disease, but caution should be exercised and such action
kept within the bounds of safety, intermitting when necessary. As in
the use of. this active agent in any disease, the first exposures should be
cautiously given, with a tube of low to medium vacuum, at 10 inches
distance, and for five minutes’ duration, and at intervals of three to
four days. After a period of ten days to two weeks, if no susceptibility
has been shown, the distance can be gradually reduced to 3 or 4
inches, and the time lengthened to ten or fifteen minutes, and the ex
posures made at more frequent intervals. The inexperienced, however,
cannot be too cautious in the bolder use of this method, as its effects
when carelessly pushed are sometimes unpleasant, not to say disastrous.
In those instances where moderate reaction has been purposely provoked
and kept up, after a few weeks’ treatment it should be discontinued till
this subsides; in some cases improvement sets in and continues. The
method should again be resumed as soon as improvement begins to flag.
Wickham, an expert in the use of radium, has had remarkable results
from its use in this disease.
Of the various methods mentioned, I personally give preference
to pyrogallol and arsenical ointments or pastes, to curetting with sup
plementary cauterization, and to x-ray and Finsen phototherapy—the
last only in rare instances and selected cases, owing to the difficulties of
its proper employment.
Treatment of lupus of the mucous membranes must be more or less
limited in its methods, owing to the difficulty of application. Curetting
can be made use of, especially when the disease is readily reached and
within easy view, and supplementary cauterization with silver nitrate
stick or strong solution. The best method, however, here consists in
1 See under General Remarks on Treatment regarding apparatus, protection of
patient, and other points.
LUPUS ERYTHEMATOSUS
753
cauterization by means of the galvanocautery, repeating at intervals
of a few weeks until the morbid tissue is all destroyed. The Paquelin
cautery may also be employed for this purpose, but is not so valuable
or generally useful as the galvanocautery. At Finsen’s institute they
make a daily application of a compound solution of iodin and potassium
iodid, and twice weekly galvanocauterization. The Pfannenstiel1 method
of treatment of intranasal cavities has been commended—consisting of
daily packing with tampons which are kept constantly moistened with
hydrogen peroxid solution, and at the same time the patient taking
sodium iodid internally. Lactic acid is a valuable remedy in these
cases, and can be applied pure, or with one to several parts water, ac
cording to whether it is used alone or with preceding curetting, and also
upon the character and infiltration of the area to be treated. Various
other remedies have been advocated from time to time, but the most
valuable, in my judgment, are curetting, galvanocauterization, and
lactic acid. The use of cocain solution as a preliminary in those who bear
pain poorly, carefully employed, reduces the pain of treatment and avoids
the necessity of a general anesthetic. The x-ray has a value in these
cases also.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |