| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
LEPRA2
Synonyms.—Leprosy; Lepra Arabum; Elephantiasis Græcorum; Leontiasis;
Satyriasis; Fr., La lèpre; Ger., Der Aussatz; Norwegian, Spedalskhed.
Definition.—Lepra is an endemic, chronic, malignant, constitu
tional disease, due to a specific bacillus, characterized by alterations in
the cutaneous, nerve, and bone structures, varying in its morbid mani
festations according to whether the skin, nerves, or other tissues are
predominantly involved, and resulting in anesthesia, ulceration, necrosis,
general atrophy, and deformity.
Ill-defined records of the existence of this malady are to be found
as far back as the remotest ages. Although its primary origin is unknown
it is not improbable, that it was in its earliest history limited to Egypt
and the Orient. Mention, sometimes of an indefinite character, is made
of it in several parts of the earlier books of the Bible.3 During the middle
ages it was quite rife in Europe, England, and Scotland, declining in the
fifteenth century and practically disappearing by the sixteenth. In
the last hundred years there seems to have been, in certain places, signs
of recrudescence, and the malady has appeared in parts where it had
1A review of the literature of x-ray in the leukemias, with bibliography, will be
found in a paper by Pancoast, in Univ. Pa. Med. Bull., Jan., 1907; and Stengel and
Pancoast, “The Treatment of Leukaemia and Pseudoleukæmia with X-rays,” Jour.
Amer. Med. Assoc, Sept., 28, 1912, p. 1166—in former over long bones, in latter over
glandular enlargements.
2 Important general literature: Danielssen and Boeck, Traite de la Spedalskhed,
Paris, 1848; Vandyke Carter, “Leprosy and Elephantiasis,” 1874; Leloir, “Traité
pratique et théorique de la Lèpre,” Paris, 1886; Thin, “Leprosy,” London, 1891;
Journal of the Leprosy Investigating Committee, London, 1890-91; Hansen and Looft,
“Die Lepra vom klinischen und pathologischen-anatomischen Standpunkt,” Bibli-
otheca medica, D. 2, H. 2; there is an English translation by Walker, London, 1895;
Mittheilungen und Verhandlungen der Internat. Lepra Conferenz zu Berlin, 1897, Berlin,
1897-98; Lepra-Bibliotheca international; Babes, “Die Lepra,” 1901; Santon, “La
Léprose,” 1901; Verhandl. v. Inlernat. Derm. Cong., Berlin, 1904, vol. i. The transac
tions of the International Congresses on Leprosy; Lie, Archiv, 1911, cx, p. 473 (sta
tistical review, based on over 1000 cases). Other literature will be referred to in the
course of the text.
3 McEwen, in two interesting papers, “The Leprosy of the Bible in its Medical
Aspect,” The Biblical World, No. 3, Sept., 1911, and “The Leprosy of the Bible: its
Religious Aspect,” ibid., No. 5, 1911, very properly concludes that leprosy of the Bible,
as also believed by most men competent to study the subject, includes many cutaneous
affections:—“The word ‘leprosy’ did not refer ever and always to true leprosy, but
was rather a generic term covering various sorts of inflammatory skin diseases, which
rendered the one afflicted unfit to associate with others, not because his condition was
contagious as a disease, but because, by virtue of the belief among the Hebrews in the
principle today known as ‘taboo,’ it disqualified him for the worship of Jehovah,
threatened others by contact with a like disqualification, and required ceremonial
procedure for removal. When this simple, and, we believe, true explanation of biblical
leprosy is understood and accepted, a great step will be taken toward the elimination of
the irrational lepraphobia of today.”
Any one who has carefully studied the subject cannot think otherwise. More
over, I am convinced that the history of the so-called great spread of the disease in
middle Europe, England, and Scotland during the middle ages and in a century or two
gradually disappearing is similarly largely mythical, due to a hysteric wave of lep-
raphobia and ignorance in diagnosis, which resulted in placing most skin disease cases,
among which doubtless some true leprosy cases, under this ban—to remain until fear
had ceased and knowledge had increased.
LEPRA
915
never before existed. It is probable, however, that this alleged increase
or recrudescence is more apparent than real, the studies and activity of
dermatologic workers in the past several decades in regard to the disease
bringing the existent cases and facts more strongly into the foreground.
Its distribution is, however, quite extensive, although the aggregated
number of cases, as well as the percentage of state and world population,
is insignificant compared to that during the early and middle ages. It
still exists today to a variable extent in Norway and Sweden, Southern
Russia, Asia, Japan, along the coasts of Africa, some of the Central and
South American States, Mexico, Cuba, and the Sandwich Islands. It
is also found in some of the British Colonies,1 in many of the islands of the
Indian and Pacific Oceans, New Zealand, Madeira, and the West
Indies. Spain and Portugal, as well as Greece and certain parts of
Italy and France, furnish a variable number of cases.
In the United States2 the earliest cases were found in Louisiana
among the French, and in Minnesota and other Northwestern States
among the Norwegian immigrants, and a limited number in South
Carolina. It also, as known, exists in its colonies recently acquired.
In more recent years, as to be expected from our nearness to leprous
centers, imported cases, especially Chinese, have been met with in
California and the other nearby Coast States. Isolated cases in indi
viduals who have contracted the disease elsewhere are also encountered
from time to time in New York, Philadelphia, Chicago, and other cities.
Symptoms.—Leprosy presents varied and manifold symptoms.
The clinical aspects in some cases seem totally different from those
in others, and in others again are frequently of mixed character. There
are, too, in most instances, several stages of the malady, which are,
however, often ill defined. Owing to these facts it is customary, and,
upon the whole, more satisfactory as to clearness, to describe the dis
tinct types separately. Probably the best arrangement is a division
of the subject into: (1) Period of incubation; (2) period of invasion;
(3) macular type; (4) tubercular type; (5) anesthetic type; (6) mixed
type. One form usually shades slightly, moderately, or decidedly into
another, so that it can readily be understood that the manifestations of
either form may vary considerably.
1 See Abraham’s paper in Trans. Internat. Leprosy Conference.
2 D. W. Montgomery, “Leprosy in San Francisco,” Jour. Amer. Med. Assoc, July
28, 1894; Dyer, “Report on the Leprosy Question in Louisiana,” Proceedings of the
Orleans Parish Med. Soc’y, meeting of June 11, 1894; Dyer, “Endemic Leprosy in
Louisiana,” Philada. Med. Jour., Sept. 17, 1898; Jones, New Orleans Med. and Surg.
Jour., 1877-78, vol. v, p. 673; Morrow, “Matters of Dermatological Interest in Mex
ico and California,” Jour. Cutan. Dis., 1889, p. 147; Hyde, “The Distribution of Lep
rosy in North America,” Trans. Cong. Amer. Phys. and Surg., 1894 (with full bibliog
raphy); J. C. White, “Leprosy in the United States and Canada,” Trans. Internat.
Leprosy Conference, 1897, vol. i; Bracken, “Leprosy in Minnesota,” Philada. Med.
Jour., 1898, ii, p. 1309; D. W. Montgomery (a white woman who contracted leprosy
in San Francisco), Lepra, Bibliotheca internationalis, vol. 1, Fasc 4, 1900; Burnside
Foster (case contracted in Minnesota), Jour. Amer. Med. Assoc, Aug. 31, 1901; Dyer,
Jour. Amer. Med. Assoc, Nov. 7, 1903; “Origin of Louisiana Leprosy,” Med. Library
and Histor. Jour., Jan., 1904; “Leprosy in North America,” Verhandl. v. Internat.
Derm. Cong., 1904, vol. 1; Daland, “Leprosy in Hawaiian Islands,” Jour. Amer. Med.
Assoc, Nov. 7, 1903; Ewing, “Leprosy as Seen in the Philippines,” Med. Record, Dec
15, 1906; Pollitzer, “Historical Sketch of Leprosy in the United States,” Jour. Cutan.
Dis., May, 1911, p. 361.
916
NEW GROWTHS
Stage of Incubation.—This is, so far as inference from the known
facts shows, extremely variable. The absence of a recognizable pri
mary lesion necessarily limits the field of observation on this point.
It has happened, however, that in some instances the malady can be
ascribed to exposure consequent upon a short visit to a region where
it is prevalent, the affection developing a variable time after the return
home—a country free from the disease. Such observations indicate
that the period of incubation, from the time of exposure to the first
manifestations, may be short or long, varying from several months
to some years, depending, doubtless, upon the receptivity and condi
tion of the individual and upon other—unknown—factors. As illus-
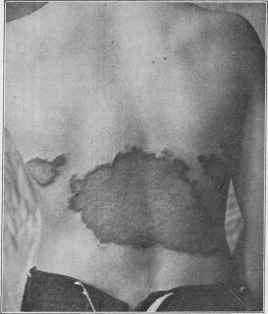
Fig. 228.—Leprosy of the maculo-anesthetic type, in a boy of fourteen; with also a
thickened macular anesthetic patch on the palm (courtesy of Dr. D. W. Montgomery).
trating the short extreme, Bidenkap, cited by Morrow,1 observed an
instance in which the disease developed a few weeks after the first
exposure, and Morrow himself had a case under his care in which the
disease appeared within ten months following a short visit to the Sand
wich Islands. On the other hand, some observers, among whom Dan-
ielssen, Boeck, and Leloir, have recorded cases having an incubation
period of ten to forty years. Doubtless the state of the health, the food
supply, climate, and surroundings, as well as the varying resisting power
of individuals, are responsible, in great part at least, for the great differ
ences in the length of time noted between exposure and the appearance
of invasion symptoms. It is not improbable, however, that in most cases
of apparent long period of incubation the disease may have already been
1 Morrow’s System, vol. iii (Dermatology), p. 566.
LEPRA
917
in existence for some time, but that the manifestations are of such mild
character that they escape observation.
Stage of Invasion.—This period varies within considerable limits,
averaging probably from several months to a year. The prodromata
of leprosy are frequently ill defined, and, unless occurring in leprous
countries or districts, and presenting something characteristic, are often
ascribed to simple ill health or considered manifestations of malaria,
tuberculosis, or some other malady. Chilliness, febrile action of an in
termittent type, malaise, disinclination to exertion, mental depression

Fig. 229.—Macular leprosy patches, associated with tubercular infiltration of the face;
same patient as Fig. 231 (courtesy of Dr. L. A. Duhring).
or hebetude, debility and epistaxis, often associated with pain, altera
tions in sensibility, and motor weakness, variously present from time to
time irregularly. One, several, or all such symptoms may be noted, but,
as a rule, those most frequently observed are the chilliness and febrile
action, lassitude and debility, and pains, especially in the extremities,
and of a more or less paroxysmal character. Instead of chilliness there
may be well-defined rigors. The fever,1 if uncomplicated, is probably
1 Lewers, “A Note on Leprous Fever,” Brit. Jour. Derm., 1899, p. 388, gives a
good brief analytic review of this subject, with citations of opinions from important
works on the disease.
918
NEW GROWTHS
always more or less intermittent, and is, as well as other symptoms, due
to the presence of the bacilli or their toxins. While often an early mani
festation, it is frequently more pronounced later, along with the appear
ance of the cutaneous symptoms. Vertigo and cephalalgia are also not
uncommon manifestations in the invasion stage. In the anesthetic
variety of the disease, while chilliness, febrile action, and some of the
other symptoms named present, there is, as is to be expected, a prepon
derance of those of a distinctly neurotic character. Morrow considers
itching, often of a severe degree, to be one of the most common and char
acteristic signs of the invasion period. Formication, sensations of
tingling and burning, pricking pain, localized soreness or tenderness, a
numb or dead feeling, heaviness, stiffness with neuralgic pain, both of a
superficial and deep character, are also variously noted.
The import of such symptoms, as well as others of the invasion stage,
is often overlooked, however, until cutaneous evidences of the malady
show themselves. In many instances, it is true, these latter are the
first signs to which the patients give attention, the earlier symptoms
having been of a mild or obscure character or practically wholly absent.
Recent studies indicate, as first pointed out by Morrow, and since em
phasized by the observations1 of Sticker, Jeanselme, and Laurens, that
the first manifestations are rather determined toward the mucous mem
branes of the pharynx and upper air-passages than toward the skin;
and betrayed by alterations of the voice, such as husky or rough phona-
tion, rhinitis with an abnormally free nasal secretion, sometimes epis-
taxis, and an increase of the salivary secretion.
Macular Type.—Macular leprosy (lepra maculosa) is to be consid
ered more as a forerunner of the tubercular form, and occasionally also
of the anesthetic variety, than as a distinct type. The eruptive mani
festations may or may not have been preceded by several or more of the
invasion symptoms. The cutaneous phenomena consist of variously
sized patches, with or without infiltration, of a red, violaceous, brownish,
or blackish color. There may be an intermingling of depigmented
vitiligo-like spots, striæ, or areas, with those of a hyperpigmented char
acter, and these all may be so ill pronounced as to give the integument
a dappled appearance. In fact, this type can be said to be sometimes
made up of a mixture of morphea-like patches, leukodermic areas, and
more or less pigmented spots and patches. Some may be atrophic,
others somewhat thickened or lardaceous and firm. The eruption may
be slight and somewhat limited, or in some instances is quite extensive.
The color may be brownish or mahogany red or sepia tint, dependent
to some extent upon the complexion and race. Occasionally it may sug
gest an ecchymosis. Patches vary in size from a pin-head to a palm or
larger, as a rule being coin to palm-sized. There is sometimes a deeper
shade centrally, in others peripherally; if the latter, the patches may
assume a distinctly circinate aspect. The skin involved may be
otherwise apparently normal, slightly atrophic or thickened, and may
show slight hyperesthesia or be more or less anesthetic. Not infre
quently irregularly scattered blebs appear from time to time, usually
1 Sticker, Jeanselme, Laurens, Trans. Internat. Leprosy Conference, Berlin, 1897.
LEPRA 919
scanty in number. The febrile and other general symptoms, already
referred to, often present at intervals, at which times there is usually an
exacerbation in the cutaneous symptoms. The malady may persist
somewhat indefinitely as this type, with sometimes paralytic motor
symptoms and sensory disturbances, with variable mixture of more
pronounced evidences of the anesthetic type; or infiltration and nodula-
tion begin to present, and it passes partially or more or less completely
into the tubercular form.
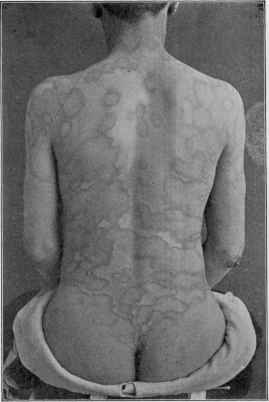
Fig. 230.—Macular Leprosy—showing unusual circinate patches (courtesy of Dr.
Howard Fox).
Tubercular Type (Tubercular Leprosy; Tuberculated or Nodular
Leprosy; Lepra Tuberculosa).—This is the more common expression of
the disease, and generally the form which is noted in a region when the
malady gains its first foothold. Later, after its existence in a community
for a long period, the milder or anesthetic type is noted to occur relatively
in greater and greater frequency. In tubercular leprosy the brunt of
the malady is seemingly borne by the integument. The earliest symp
toms are usually those described in the macular variety, which latter,
as stated, is generally to be considered an early stage of the disease.
The peculiar characters of the tubercular variety consist in the appear-
920 NEW GROWTHS
ance of tubercles and nodules, distinctly defined, or as more or less ill-
defined areas of infiltration, with subsequent ulceration. The skin,
more especially of the face, ears, and often other parts, is noted to be
thickened, seemingly hypertrophic, with an accentuation of the natural
lines. The region of the brow, particularly of the eyebrows, commonly
shows the earliest evident infiltration. Along with, as well as often
preceding, these characteristic lesions, scattered blebs and more or less
infiltrated, hyperesthetic or anesthetic, pinkish, reddish, or pale-yellow-
ish macules make their appearance from time to time, subsequently fading
away or remaining permanently.
When well advanced, the tubercular, nodular, or infiltrated masses
give rise to great deformity; the face, a favorite locality, becomes more
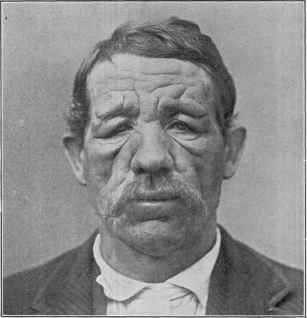
Fig. 231.—Leprosy of the tubercular type, associated with macular variety; the
tubercles not defined, but consisting of pronounced infiltration, especially about the
eyes and brow; same case as Fig. 229 (courtesy of Dr. L. A. Duhring).
or less roughly leonine in appearance (leontiasis). The hands are also
usually the seat of similar lesions, and not infrequently other regions
likewise present tubercles or areas of infiltration. As a rule, however,
the face, ears, and hands are the parts chiefly so involved.
The tubercles are brownish or brownish-yellow in color, vary in size
considerably, often attaining somewhat large proportions. They de
velop in most instances from macular, usually slightly or moderately
infiltrated, areas, although also often arising primarily upon skin seem
ingly previously unaffected. They persist almost indefinitely without
material change, or undergo absorption or ulceration; this last takes
place most commonly about the fingers and toes. Not infrequently
LEPRA 921
there is a partial or even complete disappearance of one crop of tubercles,
to be succeeded by another, and ordinarily of more pronounced char
acter. At such times the fresh outbreak is often preceded by febrile
action, chilliness, and other general symptoms. Others may undergo
some absorption and be gradually transformed into indurated, fibrous,
pseudokeloidal masses. Some may completely disappear and leave
behind atrophic, thinned, pigmented skin or cicatrices. Many tend,
however, after a more or less indefinite period, to undergo ulcerative
destruction, and this tendency, as already remarked, is most frequently
displayed with the tubercles and nodules of the extremities. The re
sulting ulcerations are of a shallow, indolent character, having a yellow-
ish-brown, viscid discharge, which sometimes dries to brownish, thickish
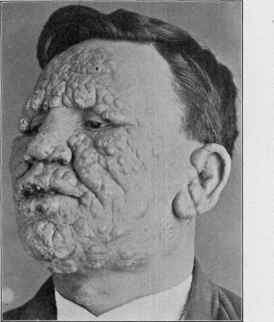
Fig. 232.—Tubercular leprosy of three years’ duration (courtesy of Dr. Howard Fox),
crusts. In some instances the ulcerative action extends deeply and may
lay bare ligaments and bones. Others after a time tend to heal, and
especially if cleanliness is maintained and antiseptic dressings applied.
In the course of time, and more particularly when ulcerative action is
pronounced, the lymphatic glands of the neck, groin, and axillæ become
enlarged, and not uncommonly finally break down and ulcerate; along
with this is noted also swelling of the lymphatics leading to these glands.
In addition to the integumentary changes, the mucous membrane
of the nares, mouth, pharynx, and other neighboring parts also shows
invasion. The eye likewise often suffers and exhibits surface tubercles
or infiltration. The hair, especially of the regions involved, sooner or
later shows impaired nutrition and falls out; this is frequently noted
922
NEW GROWTHS
about the eyebrows. The scalp hair, however, usually remains, as
this region is, according to almost all observers, peculiarly exempt from
leprous manifestations.1 The palms are likewise rarely invaded.2 The
nails do not, as a rule, seem to suffer directly, but their nutrition, as is
to be expected, is often impaired, and, as a result, there may be thinning
or thickening, irregularity, brittleness, opacity, etc There is commonly,
early in the malady, a disturbance of the functions of the sweat and
sebaceous glands; primarily there is often increased activity, but later
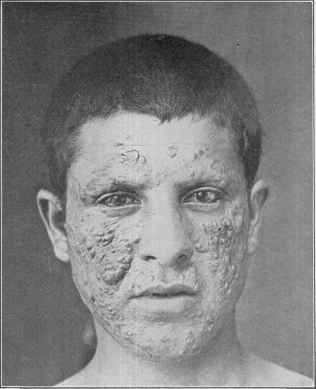
Fig. 233.—Leprosy, tubercular variety; lesions are also shown upon the cornea (courtesy
of Dr. J. A. Fordyce).
there is a partial or more or less complete arrest, and this may be localized
or somewhat general.
Anesthetic Type (Lepra Anæsthetica; Lepra Nervorum.—Anes
thetic leprosy, in which the brunt of the malady is borne by the nervous
system, is characterized chiefly by anesthetic and atrophic manifesta-
1 Morrow, “A Case of Macular Lepride of the Scalp—with Remarks on the Locali
zation of Leprous Lesions,” Jour. Cutan. Dis., 1900, p. 10, reports a case in which the
scalp showed macular manifestations; Pernet, Brit. Med. Jour., Nov. 11, 1905, p. 1280,
reports 2 cases in which the scalp was involved.
2 D. W. Montgomery, Jour. Cutan. Dis., 1899, p. 445, noted an instance with a
maculo-anesthetic leprid upon the palm; a case with a similar circinate patch in this
region, in addition to manifestations on other parts, recently came under my notice.
LEPRA 923
tions. The latter are usually more or less limited to the hands, feet, and
face. Its development is an insidious one, and it is not infrequently a
part of or a sequence of the macular form. Following or along with the
precursory symptoms denoting general systemic disturbance, or inde
pendently of any prodromal indications, a hyperesthetic condition, in
localized areas or more or less general, is observed. As a rule, febrile
attacks, or the pseudomalarial aspect, is not a usual, or at least not so
constant, accompaniment of this type. Lancinating pains along the
nerves, particularly of the extremities, and an irregular, scattered, pemphi-
goid eruption are, however, commonly noted. The malady may present
nothing further than these various manifestations, often along with
occasional attacks of, or more or less persistent, pruritus, for an indefi
nite time, ordinarily one to several years. Sooner or later there follows
the special eruption, coming out from time to time, and consisting of sev
eral or more, usually non-elevated, well-defined, pale-yellowish patches,
1 or 2 inches in diameter. They rarely present in numbers, but gen
erally present singly, new areas appearing from time to time. They
are found most frequently upon the back, shoulders, dorsal surface
of the arms, thighs, about the elbows, knees, and ankles. The face
also may show the eruption. There is often a symmetric distribution.
Leloir noted an instance of double zoster-like arrangement on the chest.
As a rule, they are at first neither hyperesthetic nor anesthetic, but may
be the seat of slight burning or itching. They spread peripherally, and
tend to clear in the center. The patches eventually become markedly
anesthetic, and the overlying skin and the skin on other parts as well
becomes atrophic and of a brownish or yellowish color. In many in
stances when first appearing they are of a sepia-brown shade, and some
times of a bluish-red color, and usually more pronounced at the border
portion. Occasionally if several are close together coalescence gradually
takes place, resulting in gyrate patches, with a well-defined, sometimes
slightly elevated, reddish periphery, and a pale or leukodermic atrophic
central portion. In fact, instead of the eruption presenting itself as
yellowish-brown areas, of the features described, the earliest patches may
be of a vitiligo-like character. In some cases there is depigmentation,
extending over considerable surface.
The areas are frequently preceded by sensory disturbance, such as
formication, burning, or stinging sensations. While they are in their
first appearance sometimes hyperesthetic, after a variable time, usually
soon afterward, there is anesthesia, especially centrally. Not uncom
monly the central portion becomes anesthetic, while hyperesthesia is
noted in the spreading border. In some cases, or in some stages of the
malady, the anesthesia does not confine itself to the immediate areas,
but may involve considerable surface, or even an entire region supplied
by an affected nerve. While ordinarily the nervous disturbance primar
ily does not compromise the tactile sense, consisting at such period of
hyperesthesia, analgesia, and thermo-anesthesia, later the sensory func
tions are wholly abolished.
As the disease continues and the nerve involvement becomes more
pronounced atrophic symptoms are noted to ensue. The subcuta-
924
NEW GROWTHS
neous tissues, muscle, hair, and nails undergo atrophic or degenerative
changes, and these changes are especially observed about the hands
and feet. These parts become crooked, thinned, emaciated, and other
wise distorted. Surface ulcers appear, either spontaneously or as the
result of knocks or other injuries. The muscles atrophy, the fingers
become drawn up and flexed, producing the so-called “leper claw.’’
Finally the bone tissues are involved, the phalanges dropping off or dis
appearing by disintegration or absorption (lepra mutilans). The toes
and feet are similarly affected, and not infrequently, especially in those
who go barefooted, a deep plantar ulcer forms. The process may not
stop at disintegration and destruction of the fingers and toes, but the
hands and feet may gradually be wholly lost. The ulnar and peroneal
nerves and other nerves of
the extremities seem to be
especially prone to the damag
ing influence of the bacillus
invasion. The ulnar nerve
particularly is considerably
thickened, either uniformly or
irregularly, and can usually be
felt as a thick, tense cord, and
is often painful upon pressure.
In addition, owing partly to
the atrophy of the glandular
structures and the consequent
suppression of the sweat and
sebaceous secretions, there is
often a thinned, atrophic-look-
ing condition of the skin of the
arms and legs, which is gen
erally of a dirty yellowish or
brownish color, and presents
a somewhat tense appearance,
and with thin, flaky, or branny
scaliness. Occasionally the
skin is somewhat wrinkled.
In occasional cases the skin of
the trunk likewise exhibits similar changes. The atrophic action also
often involves the face, and along with the paralytic symptoms, which
sooner or later presents, give rise to considerable facial disfigurement.
The face is sometimes drawn to one side. The eyelid muscles are often
involved, and, in consequence, and also partly owing to the loss of
eyelashes, the eyes not being properly protected, inflammation, ulcera-
tion, and opacities ensue.
Ulcerations are not so common a feature of the anesthetic as of
the tubercular form, and are chiefly the result of trophic influence,
arising principally from dry or moist gangrene, and from knocks or
other injuries.
The mucous membrane, especially of the mouth, soft palate, uvula,

Fig. 234.—Leprosy of the tubercular type,
on face, associated with anesthetic type; same
case as Figs. 235 and 238.
LEPRA
925
and back of the pharynx, shows loss of sensibility and other nervous
disturbance, and there is serious interference with the act of deglutition,
often giving rise to regurgitation through the nostrils.
Mixed Type.—The mixed form of leprosy is, as the name signifies,
characterized by features of the several types described. The early le
sions are usually, as in the other forms, those of the macular type. Later
there is often at first the development into the anesthetic or tubercular
expression of the disease, and which may persist as such for a variable
time, and then gradually
present symptoms of the
other variety. The dis
tinctly anesthetic form of
the malady may, there
fore, sometimes sooner or
later have added tuber
cular and nodular infiltra
tions, and with subse
quent ulceration; the tu
bercular form likewise may
present after a time fea
tures of the anesthetic
type, not infrequently,
however, the clinical fea
tures are of mixed char
acter from the beginning.
Course.—Leprosy
runs a chronic persistent
course, with, in many
cases, remissions, or even
temporary or more or less
prolonged intermissions.
Exacerbations in the cu
taneous phenomena occur
from time to time, and
at such periods there are
generally preceding and
accompanying constitu
tional symptoms of mal
aise, debility, febrile ac
tion, and chilliness or
distinct rigors. These are much less common, however, in the anes
thetic variety, and not infrequently are practically absent. The in
tegumentary lesions become slowly more pronounced and numerous, and
while the tubercles and nodular masses and infiltration may undergo
absorption, new outbreaks predominate over retrogressive changes.
More commonly these lesions show ulcerative changes. The nervous
form of the disease, as already described, increases, as a rule, steadily,
but is much less rapid in its progress than the tubercular form, usually
lasting from ten to thirty years, averaging probably twelve to fifteen.
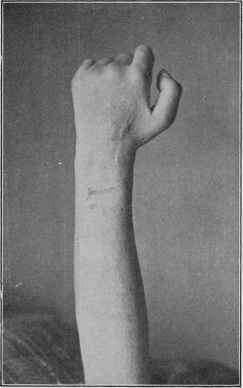
Fig. 235.—Leprosy, showing paralysis and atro
phy of some of the extensor muscles, and the “leper
claw” of the anesthetic type; faint macular anes
thetic area shows on forearm; same case as pre
ceding, with tubercular type on face.
926 NEW GROWTHS
In tubercular leprosy death results in almost half the cases from
the direct effect of the disease, either from exhaustion or involvement
of the air-passages or of internal organs. Renal and lung complications

Fig. 236.—Anesthetic leprosy—showing “claw hand” with ulcerations (courtesy of
Dr. J.M.Winfield).
carry off almost as great a number. The remainder die from anemia,
or enteric complications with colliquative diarrhea. In the anesthetic
form the end comes from the direct action of the leprous poison, from

Fig. 237.—Anesthetic leprosy, showing characteristic mutilation (courtesy of Dr. J. M.
Winfield).
exhaustion, muco-enteritis, long-continued digestive disorders, or other
complications. Pulmonary and renal disorders are not encountered
as often in this form as in the tubercular variety.
LEPRA
927
It is not improbable, however, that the pulmonary and enteric
maladies which bring the fatal end in leprosy cases are, in reality, not
complications, as usually understood, but are themselves of leprous
character. Arning believes that the supposed intercurrent pneumonia
and tuberculosis, and the diarrhea or dysentery, are due to leprous
infiltration—which he denominates respectively phthisis leprosa and
enteritis leprosa. Beaven Rake’s1 conclusions are practically the same.
The culture experiments with fragments of assumedly phthisical lung
or tuberculous viscera from lepers have, as he states,2 so far been unsuc
cessful, this tending to confirm the view that these conditions are lep
rous and not really tuberculous. As to kidney complication, this same
observer3 found, in 78 autopsies, some form of nephritis in 23 cases, a
percentage of 29.4. He noted a much longer duration of life in these
cases when occurring in the anesthetic variety than in the tubercular

Fig. 238.—Leprosy, with paralysis and atrophy of extensor muscles, and some small
ulcerations on toes, and slightly scurfy skin; same case as Fig. 235.
form, which he attributes to the fact that in the latter variety the sweat-
glands are involved earlier and to a more serious extent, thus throwing
more strain on the kidneys.
Etiology.—The direct cause of leprosy is now accepted to be
a specific bacillus—the bacillus lepræ. The discovery by Hansen, in
1874, has completely negatived the hereditary theory formerly so strongly
held. It is true that the evidence points to the fact that certain individ
uals or families may, as likewise now believed regarding tuberculosis, show
a readier susceptibility when exposed to invasion. It is certain, too,
1Beaven Rake, “The Significance of Visceral Tuberculosis in Leprosy,” Brit. Jour.
Derm., 1890, p. 33 (based upon a study of 90 autopsies).
2 Beaven Rake, Brit. Med. Jour., Aug. 4, 1888.
3 Beaven Rake, “The Kidney Lesions in Leprosy Considered in Relation to the Skin
Changes,” Brit. Jour. Derm., 1889, p. 213 (with citation of the opinion of others as to
the complication, with references).
928
NEW GROWTHS
that the liability to successful implantation of the organism is measurably
increased by such predisposing influences as climate, soil, abode, food,
and habits. It is known that the malady is most prevalent in tropical
and subtropical countries, although it is also common in some cold
climates, as Norway, Iceland, and elsewhere. It is, moreover, distinctly
a disease of the coast and nearby waterways; it also occurs, however,
inland, and in high regions likewise, although to a relatively slight extent.
The method by which the organism gains access is not known.1
Recent observations (Morrow, Sticker, Jeanselme, Laurens, Babes,
von Peterson, Flügge, Besnier, Glück, Schaeffer) indicate that the
mucous membrane of the nose, and probably of the mouth also, may
be a not uncommon source of communication and infection.2 Schaeffer3
refers to experiments on this point. Slides were placed in the vicinity
of leprosy patients while they were reading aloud, and subsequently
examined, disclosing the presence of large numbers of bacilli. It is not
improbable, also, that entrance may take place through some abrasion
in the skin (Lassar, Arning, von Peterson, Ehlers, Geill). Geill4 calls
attention to the fact that in tropical countries, with the people who go
barefooted, the first lesions are seen frequently upon the feet—in 50
per cent, of his own cases. It is known that the bacilli can be found
in the feces (Boeck).5 Vaccination has exceptionally been blamed for
the introduction of the organisms, but there is scant reliable evidence
on this point.6 There is a growing belief that the malady is not directly
contagious or inoculable from man to man, but that there is an inter
mediate host, or insect carrier, as now generally believed as to malaria,
and it is one that might explain many apparent contradictions.7 Hutch-
inson8 has long held, as is well known, the opinion that in the eating of
fish, especially raw or salted, is to be found the cause of the malady;
lately he has added the suggestion that the bacillus may gain access in
1 See Morrow’s interesting paper, “Sources and Modes of Infection in Leprosy,”
Trans. Amer. Derm. Assoc. for 1899, p. 113; Mugliston, Jour. Trop. Med., 1905, p. 209,
suggests that the itch mite may possibly be the means of communication—having the
leprous bacillus in or simply on its tissues when it enters the skin.
2 Mewborn, Jour. Cutan. Dis., 1903, p. 23ó, found numerous bacilli in the nasal
secretion taken from a case observed by Fordyce.
3 Schaeffer, Trans. Internat. Leprosy Conference, Berlin, 1897.
4 Geill, ibid.
5 Boeck, Festschrift, Unna (1910, Bid. 1, p, 436), and Dermatolog. Wochenschr., Oct.,
1912, lv, p. 1267 (discusses the possibilities of spread of disease by this source).
6 See Baum’s paper, “Leprosy and Vaccination,” Med. Standard, 1893, p. 163.
7 Goodhue (Boston Med. and Surg. Jour., 1906, vol. cliv, p. 357) states that he has
found the bacillus in the bedbug and in the mosquito, but as yet this statement remains
without corroboration by others; Currie, “Mosquitoes and Fleas in Relation to the
Transmission of Leprosy,” Public Health Bull., 1910, Washington, D. C. (full abs.
in Jour. Trop. Med., May 1, 1911), made some experiments in the laboratory at Hono
lulu, with the results: mosquito, chiefly culex cubensis, negative, as the proboscis is
inserted into a blood-vessel obtaining bacilli—free blood; domestic flies will convey the
bacillus from a discharging leprous ulcer to the skin of a healthy person in the neighbor
hood; Engelbreth (Dermatolog. Wochenschr., 1912, liv, pp. 700 and 723), in an interesting
paper on the origin of the disease, endeavors to show that leprosy has flourished in all
countries where the goat flourished, and tends to disappear where these give way to the
breeding of sheep and cattle; he believes that an internal disease in the goat, closely
resembling tuberculosis, is transmitted to man (through milk, etc), and results in
leprosy.
8 Hutchinson, “Leprosy and Fish-Eating,” London, 1906.
LEPRA
929
this way. His views as to this food-cause are negatived by the general
observations of others. It is not at all unlikely, however, that its en
trance, in some cases at least, may be through the food.
While one, upon going thoroughly over the clinical evidence, must
admit the communicability of the disease, yet there are other unknown
factors in addition to the active one—the bacillus—which seem to be
necessary. Hereditary tissue weakness, climate, food, abode, and
habits are, doubtless, therefore contributing. If its successful communi-
cability depended upon the bacillus alone, the examples of the con
tagiousness of the disease should be common, instead of rare.1 Its con
tagiousness, under favoring circumstances, is shown in the rapid spread
in Hawaii, and more recently the suggestive increase in Louisiana (Dyer).2
But even in Hawaii the contributing influence of race, poor food, and
other factors is disclosed by the fact that the leper population consists
almost entirely of Hawaiians and half castes, less than 3 per cent, are
Chinese, with a few other foreigners—British, American, German, etc.—
not exceeding a dozen. As von Düring well remarks, however, all nega
tive evidence brought forward as to its non-communicability is valueless
in the face of one positive fact to the contrary. And though these posi
tive data are, in my judgment, relatively scanty, still they are sufficient
to make us look upon the existence of cases in our midst as of possible
danger, although this is in civilized, well-fed, and well-cared-for communi
ties exceedingly remote.3
It is generally admitted that the anesthetic type is not so contagious
as the tubercular; and it is also commonly believed that the form of the
disease in a community which is usually primarily tubercular, gradually,
after years, loses its virulent character somewhat, and that it subse
quently persists in the anesthetic form. Zambaco4 and a few others
would also have us believe that its virulence becomes still further atten-
1Hutchinson states (Brit. Med. Jour., June 29, 1889) that not a single sporadic
case is ever now seen in England; the cases there are all imported. Bronson says (Jour.
Cutan. Dis., 1895, p. 428) of New York: “we have had lepers in this city for many
years, and yet there is not a single case on record where local contagion has occurred.”
Lutz (ibid., 1892, p. 477), speaking of his experience and observations in South America
and the Hawaiian Islands, says: “Contagion even by intimate and prolonged contact
is by no means frequent in families living in a civilized way and in easy circumstances.”
Hallopeau (Trans. Internat. Leprosy Conference, Berlin, 1897) says that “in Paris up to
the present no case has been known to arise there”; and Besnier (ibid.) also states
that “in Paris, at the Hôpital St. Louis, lepers are not isolated, and notwithstanding
this no instances of contagion have ever occurred”; Thompson (Lancet, Mar. 5, 1898)
shows that in Victoria and Australia, where lepers have mingled freely with the com
munity, the disease is on the decrease. Kaposi (Wiener klin. Wochenschr., No. 45,
1898), while admitting that from a pathologic point of view the malady is infectious,
holds that clinically it is not contagious. Zambaco, who is still a champion of the hered
itary nature of the disease, states that he has never seen a case originating in contagion.
2 Dyer, Philada. Med. Jour., Sept. 17, 1898.
3 Bracken, ibid., Dec 17, 1898, states that it is quite possible, judging from his
own observations, for leprosy to die out in certain favored sections of our country,
such as Minnesota, without segregation, provided the importation of lepers be dis
continued.
4 Zambaco, Trans. Internat. Leprosy Conference, Berlin, 1897; see also Leloir’s
interesting paper on this point, “Existe-t-il dans des pays réputés non lépreux, en France
et en particulier dans la region du nord et a Paris, des vestiges de l’ancienne lépre,”
Bull, de l' Acad. de Méd., Paris, 1893, p. 215; a good abstract in Brit. Jour. Derm., 1893,
p. 129; see also references under Morvan’s disease.
59
930 NEW GROWTHS
uated, and that the disease is finally exemplified in many cases of the
maladies known as syringomyelia, scleroderma, morphea, sclerodactylia,
Raynaud’s disease, and progressive muscular atrophy (Aran-Duchenne),
considering them to be modified or weakened forms of lepra.
Pathology.—The bacillus is now fully accorded the rôle of
starting and producing the pathologic changes, and which has in
recent years received considerable study by many investigators. The
bacillus is a slender, rod-like, straight or very slightly curved parasite,
averaging about 1/5000 inch in length (from one-half to three-fourths
the diameter of a red blood-corpuscle); and its thickness is about one-
fourth to one-fifth of its length. According to Cornil, the longest are
found in parenchymatous organs, while those found in the skin nodules,
owing to compression, are, as regards size, less developed. Morpholog
ically they are very similar to tubercle bacilli, and their differentiation
is not always easy. Lepra bacilli are, however, in relatively greater
abundance in the tissues, usually occur in clumps, groups, or masses,
are smaller and less uniform in diameter than the tubercle bacilli. They
also exhibit readier reaction to staining agents, “dependent upon micro-
chemical reaction of the investing membrane of the bacillus to acids,
alkaline and anilin dyes.” They are best demonstrated by staining the
section of tissue or débris of a broken-down nodule by Ehrlich’s process
with fuchsin, and methyl-blue as a contrast (Crocker). While the
bacilli are sometimes found more or less generally distributed in the
tissues, they have certain predilections. They are usually most abundant
in the diffuse and nodular infiltrations, in the connective tissue of the
peripheral nerves, in the lymphatic glands and spaces, and sebaceous
glands (Babes and Unna); but are rarely to be found in the true maculo-
anesthetic patches, unless associated with some infiltration. They are
also found in the liver, spleen, kidneys, in the testicles (Neisser and
others), and, according to Arning, also in the ovary. In fact, in well-
advanced cases, more especially in the tubercular form, scarcely any
organ escapes. The physiologic secretions remain free so long as the
secreting tissue or membrane does not become the seat of leprous de
posits. The blood-vessels, except those peripherally involved in the
leprous infiltrations or in the last stages of the disease, rarely contain
bacilli.
The earlier reports (Campana and Ducrey, Hansen, Neisser, Carras-
quilla, Van Houtum and Emile-Weil) of alleged moderately successful
culture of the bacillus have been looked upon with considerable question;
but the later trials (Kedrowski, Clegg, Duval, Brinckerhoff, Currie and
Holman, and others) seem to have been more fortunate, but with some
slight puzzling diversity in the results. Duval and Wellman,1 from a
1 Duval and Wellman (“A Critical Study of the Organisms Cultivated from the Le
sions of Human Leprosy, with a Consideration of their Etiologic Significance,” Jour.
Cutan. Dis., 1912,p. 397), as a result of their own researches, reached the following con
clusions: (1) From a bacteriologic study of 29 cases of leprosy, an acid-fast bacillus was
discovered in 22. (2) A chromogenic strain similar in all essentials to that described by
Clegg was recovered from 14 cases, which under certain conditions grows as (a) non-
acid-fast streptothrix, (6) non-acid-fast diphtheroid, and (c) an acid-fast bacillus. (3)
Eight cases yielded an organism which was distinctly different from Clegg’s bacillus in
its biologic character, growing only upon special medium and not producing pigment.
LEPRA
931
review of the subject and their own investigations, conclude that two,
possibly three, different organisms have been cultivated from the specific
lesions of leprosy, namely: (1) a non-acid-fast diphtheroid (Kedrowski),
(2) an acid-fast chromogenic bacillus (Clegg), and (3) a permanently
acid-fast bacillus (Duval). Williams has grown four different types of
organisms, including a Gram-positive non-acid-fast streptothrix, which,
however, he believes to be different phases of the same organism. The
earlier experimental animal inoculations (Hansen, Köbner, Damsch,
Rake, Campana, Profeta, Vossius and Melcher-Orthmann) were, accord
ing to Neisser’s examination of the question, practically negative; in a
few instances there was a suspicious local growth. More recently Duval
and Gurd, Sugai, Monobe, Bayon, Rost and Williams, and others seem
to have succeeded in producing the disease, or at least conditions simulat
ing it, in the Japanese dancing mice, white mice, rats, and monkeys—
in most of these later instances the inoculating material consisted of the
cultured organism.1 According to Duval and Gurd the bacilli may live
for more than a year outside of the body. The reported successful inocu
lation (Arning) some years ago in man must be viewed with suspicion,
inasmuch as the subject belonged to a leprous family.
If a section of recent nodule is examined, it is observed to consist
(Neisser) of a cell-mass separated by sparse fibrillary intermediate
tissue; the cellular elements, mostly rounded in form and primarily like
lymph-corpuscles, undergo increase in size and reach four or five times
their original volume, constituting the so-called lepra cells and the giant-
cells found in leprous tissue. The nucleus, likewise, shows similar in-
(4) Animal experiments undertaken for the purpose of differentiating the two types
removed from the human leprous lesion and to fix their etiologic status were not re
garded as conclusive. (5) Serologic tests, especially those performed with highly
immune sera, suggested that the bacillus of Clegg was not related to Duval’s non-
chromogenic, slow-growing culture of leprosy. (6) The rôle played by the chromogenic
bacillus of Clegg in the production of leprosy was unsettled. (7) The non-chromogenic
strain, while behaving according to most of our notions of a pathogenic organism, had
not yet been proved to be the cause of leprosy, although it was probable that it might
be so, and the writers considered that it deserved more serious attention than any strain
cultivated from the human leprous lesion. (8) The wide variation in morphology and
staining reactions for certain cultures which subsequently become rapid growers and
chromogenic explained that interpretation of European writers, that the Bacillus lepræ
is a bacterium of such pleomorphism that it can be recognized as a diphtheroid, a
streptothrix, and an acid-fast bacillus.
1 The reader desirous of pursuing further the subject of cultures and inoculation
experiments is referred to the following additional contributions: Macleod, “A Brief
Survey on the Present State of Our Knowledge of the Bacteriology and Pathologic
Anatomy of Leprosy,’’ Brit. Jour. Derm., 1909, p. 309; Sugai, Lepra, 1909, viii, p. 203;
Clegg, Philippine Jour. Sci., 1909, iv, p. 403; Duval Jour. Exper. Med., 1910, xii, p.
649, and 1911, xiii, p. 365; and “The Experimental Production of Leprosy in the Mon
key (Macacus rhesus),” with review, Penna. Med. Bull., 1911, p. 665; Duval and Gurd,
Arch. Int. Med., 1911, vii, p. 230, and “Experimental Leprosy and Its Bearing on
Serum Therapy,” Jour. Cutan. Dis., 1911, p. 274; Currie, Clegg, and Holman, “Studies
upon Leprosy: Cultivation of the Bacillus of Leprosy,” Public Health Bulletin, Sept.,
1911, No. 47, Washington, D. C, p. 3, (chronologic review of literature and their
own work); Bayon, Jour. London School Tropical Med., 1911, 1, p. 45; and Brit. Med.
Jour., Feb., 24, 1912; Alderson, “Artificial Cultivation of Lepra Bacillus in Hawaii,”
California State Med. Jour., 1911, ix, No. 3; Rost and Williams, “Scientific Memoirs of
Gov’t. of India,” 1911, No. 42—abs. in Brit. Jour. Derm., 1912, p. 164; Williams,
Indian Med. Gaz., “Review Editorial,” Lancet, 1912, clxxi, No. 4584; Monobe, Japan-
ische Zeitsch. für Derm, und Urol., Feb., 1912, xii, No. 2, p. 8—abs. in Jour. Cutan.
Dis., 1912, p. 449.
932
NEW GROWTHS
crease, and some cells may contain several nuclei. The cells are most
plentiful in the neighborhood of the blood-vessels, which are numerous
and the vascular supply abundant. Leprous growths are, however, less
vascular than ordinary granulation tissue, and therefore undergo retro
gressive changes more slowly. The epidermis is not involved in the
specific morbid process, and never contains the parasites. The his-
topathologic changes are especially noted in the papillary layer, in the
main body of the corium and the subjacent tissue. According to Neisser
and others, a lepra tubercle or nodule is primarily composed of granula
tion cells. The deepest cellular layer, that in the subcutaneous tissue,
is noted to contain, along with many unchanged lymph-cells, the smallest
and most recent tumor cells, and but relatively few bacilli. The cells
show gradual enlargement in the higher layers. The oldest, topmost,
layers are divided from the rete by a stratum of subepidermal connective
tissue; the epithelial layer, except as to the disappearance of its inter-
papillary dippings, is otherwise normal, although showing increased
pigmentation. More especially in the upper layers of the tumor are
seen peculiar large, rounded, sharply circumscribed accumulations, the
so-called “globi,” composed of cells very densely infiltrated with bacilli
and their products, and undergoing degeneration. Besides the large
lepra cells there are small cells apparently identical with migratory
cells; and small connective tissue cells which show here and there en
largement from infiltration with bacilli.
There is a difference of opinion as to whether the bacilli lie within
or without the cells. Virchow, Neisser, and almost all others consider
that they are almost exclusively within the large round lepra cells,
whereas Unna,1 Herman,2 and a few others maintain that they are
chiefly found in lymph-spaces, Unna asserting that the lepra cell is
nothing more than a glœa-like mass formed by degeneration of the bacilli.
It is now recognized that a large proportion of the bacilli found in the
tissues are dead; that even in young newly formed lepromata dead
bacilli occur, while in older lesions the majority of the bacilli are dead
(Macleod). Virchow believed the fixed connectivetissue cells to be
the mother-cells of the subsequent granulation tumor. Thin and
Neisser hold the view that the lepra cells develop from emigrated white
blood and lymph-corpuscles.
In the anesthetic variety the chief changes are in the nerves. Vir-
chow, Neisser, and others place the primary pathologic process in the
peripheral and cutaneous nerves, due to leprous new formation, leading
to compression and atrophy of the sensory and trophic fibers. The
nerves most frequently affected are the ulnar, median, radial, musculo-
cutaneous, intercostal, humeral, and peroneal. It is generally believed
that these changes are practically limited to the peripheral nerves,
Hansen, Hillis, Leloir, Neisser, and others finding the spinal cord and
brain, in the cases examined by them, normal. In more recent years,
however, several observations seem to point to the possibility of central
1 Unna, Histopathology.
2 Herman, “The Bacillus of Leprosy in the Human System at Different Periods of
its Growth,” Trans. Internat. Leprosy Conference, 1897.
LEPRA 933
nerve involvement; Chassiotis1 found in one instance investigated by him
bacilli in the spinal cord.
Diagnosis.—The recognition of a well-developed case of lep
rosy of either type is, as a rule, not attended with difficulty. It is an
entirely different matter, however, in many instances in the earlier
stages, or in those of advanced period if the disease is atypical.2 In the
invasion and early eruptive stage the prodromal symptoms of chilliness,
febrile action, with subsequent free perspiration, so often observed in
the tubercular form, may be, and often are, confounded with those of
malaria. The erythematous areas may be confused with simple ery
thema, although they are commonly larger, frequently tend to show in
filtration, and are slow in undergoing involution. If to these symptoms
could be added sensory disorders, usual in anesthetic leprosy, together
with a history of exposure, a strong suspicion could be entertained, and
probably a positive opinion reached.
In the anesthetic variety the prodromal symptoms are also usually
of variable character and intensity, and the pain and motor weakness
often attributed to rheumatism or neuralgia; the other disorders of sen
sation, such as hyperesthesia, sensations of burning, tingling, numbness,
formication, and pruritus, one or several of which may be present, are
often wrongly interpreted as pointing to neurasthenia or other nervous
disorders. When, however, such a patient is living or has been living
in a district where the disease prevails, the possibility of leprosy is to be
borne in mind. This would be materially strengthened by the presenta
tion of erythematous patches of a dull red color, and of persistent char
acter, with a tendency to clear centrally while extending at the border,
the central part generally becoming whiter than normal and anesthetic.
Such areas are, however, to be distinguished from those of morphea and
vitiligo.
Later in the course of the malady the tubercular form is to be differ
entiated mainly from lupus vulgaris, the tubercular syphiloderm, and
granuloma fungoides. In the first the eruption is usually quite limited,
at least relatively, and most commonly confined to a portion of the face,
is of slow development, and frequently spreads from one center. More
over, it, as a rule, lacks the infiltration generally noted in leprosy. The
tubercular syphiloderm is also a limited eruption, and differs materially
from that of leprosy by the fact that it tends to occur in segmental,
crescentic groups or serpiginous tracts—a formation rarely, if ever,
noted in leprous infiltrations or tubercles. Both lupus and syphilis are,
moreover, ordinarily wanting in any suspicious prodromal symptoms.
Granuloma fungoides and well-marked tubercular leprosy have also
sufficient in common to give rise to possible confusion, but the early
eczematoid manifestations of the former, with the usually accompanying
itchiness, its more general distribution, the brighter red color, often serve
to differentiate; in the later stage the peculiar fungoidal ulcers would be
distinctive.
1 Chassiotis, “Ueber die bei der anästhetischen Lepra in Rückenmarke vorkom-
menden Bacillen,” Monatschefte, 1887, vol. vi, p. 1039.
2 Thin (loc. cit.) cites numerous examples of errors in diagnosis by observers experi
enced in dermatology.
934
NEW GROWTHS
The anesthetic form in the more advanced stages is to be distin
guished chiefly from syringomyelia, to which it sometimes bears a
striking similarity. The various sensory disorders, however, when
taken together with the lesions of the bones and joints of the extrem
ities, with the mutilations and deformities, commonly observed in ad
vanced stages of leprosy, with the history, often, of preceding pem-
phigoid eruption, and vitiligo or morphea-like patches, are quite char
acteristic.
In cases of doubtful nature, whatever the type of the malady, the
final decision is often to be based upon the presence of the special bacillus,
as determined by repeated examinations. Shepherd1 advises, when
the question of immediate diagnosis is one of great urgency, cutting
down on the ulnar nerve, removing a portion, and examining for bacilli.
It is commonly believed that leprous patients give a positive Wasser-
mann, but there are exceptions to this.2
Prognosis.—The outlook for leprosy patients is unfavorable, a
fatal termination, with occasional exceptions, being the rule, although
the end may not be reached for a number of years. The tubercular form
is the most grave, the mixed variety the next, and the anesthetic the
least. The statistics of the Trinidad Asylum, according to Rake,3 show
that the average duration is eight and one-half years. In some instances,
especially of the anesthetic variety, it may be fifteen to twenty years
or more. Patients are not infrequently carried off by intercurrent
disease, although, as already referred to, apparently independent organic
affections are often, in fact, due to leprous invasion and infiltration.
Under the most favorable conditions much can be done, and doubtless
an occasional cure—a symptomatic cure at least—brought about.
There seems scarcely question that mild or abortive types occur,
though doubtless but rarely. Hansen and Looft, in quoting Daniels-
sen’s observations as to the Norwegian hospital, “that the results of
treatment were nothing to boast of, but show that leprosy at its com
mencement can be cured,'’ add the reservation “that the cure is not due
to the treatment, but to the natural development of the disease.” One
cannot go over the literature without recognizing the fact that in excep
tional instances patients recover, or at all events the malady remains
permanently quiescent. Impey4 is strongly of the opinion that some
cases, especially the anesthetic, undergo spontaneous cure, and believes
that in many so-called lepers the malady has already run its course, and
that the effects alone remain, and may go on from the damage done the
nerves. He quotes Hansen’s studies as showing that the latter observer
“had never found bacilli in the nerves of a chronic case, . . . and that
1 Shepherd, “Notes on a Rapid Method of Diagnosis in Leprosy,” Jour. Cutan. Dis.,
1903, p. 476.
2 Bloombergh, “The Wassermann Reaction in Syphilis, Leprosy, and Yaws,”
Philippine Jour Sci., Oct., 1911, p. 335 (doubts a positive reaction in leprosy, and thinks
before accepting the same present or antecedent frambesia and syphilis must be
excluded—of decided importance in countries where these diseases prevail; references
to pertinent papers are given).
3 Rake, Report on Leprosy in Trinidad, 1885.
4 Impey, “The Non-Contagiousness of Anesthetic Leprosy,” Trans. Internat. Lep
rosy Conference.
LEPRA
935
he had examined the bodies of many of these patients after death, and
found no bacilli in any organ.” Thin, D. W. Montgomery, G. H. Fox,
Ehlers, Hallopeau, Dyer, and others1 have in recent years reported cures
of the disease, spontaneously or as the result of treatment.
Under the most favorable circumstances of change of residence to
a non-leprous district, improved hygiene, good food, supporting and
tonic treatment, cleanliness, and aseptic applications, it seems, there
fore, not improbable that exceptionally cases get well, or at least the
disease ceases to be active.
Treatment.—The management of leprosy naturally includes a
consideration of the means of prevention. There are still great dif
ferences of opinion as to the necessity of segregation, and each side of
the question has much in its support. The conclusions of the Inter
national Leprosy Conference at Berlin, 1897, were, upon the whole,
in favor of this, with certain qualifications as to its practice, depending
upon local conditions.2 It is generally recognized that the anesthetic
cases are much less dangerous to a community than the tubercular form,
and segregation less urgent. The necessity of segregation in districts
where the cases are sparse, with no tendency to spread, and where lepers
can be properly cared for at their homes, is questioned by many of con
siderable experience. As already stated, the imported cases in Paris,
London, Vienna, Berlin, New York, Chicago, Philadelphia, and other
places where the disease is not endemic have never given rise to
others.
The treatment of leprosy has first in view the maintenance of the
patient’s general health by hygienic and other measures, and the em
ployment of such tonics as may seem demanded. The value of change
of abode to a non-leprous country, when possible, has already been
alluded to, and will in some instances stay, and probably always delay,
the progress of the malady. There are certain remedies for which
special claims have been made from time to time by different observers.3
The most important, and those which have received the greatest support,
are Chaulmoogra oil (Le Page), gurjun oil (Dougall), and nux vomica or
strychnin.
Chaulmoogra oil (oleum gynocardiæ, from the seeds of the Gyno-
cardia odorata) is given in doses varying from 5 minims (0.33) to 1½
drams (6.) or more three times daily. It is administered in milk, in
emulsion, or in capsules. As a rule, its good effects are obtained only by
the larger doses, and these cannot always be reached, owing to the fact
that the oil is so prone to disturb digestion, some persons being intolerant
1 Thin, Brit. Med. Jour., May 4, 1901, p. 1074; D. W. Montgomery, Med. Record,
April 19, 1902 (spontaneous; 6 cases); Hallopeau, Annales, 1903, p. 32; Dyer, Med.
News, July 29, 1905.
2 As especially bearing upon the control in our own country see papers by J. C.
White, “The Contagiousness and Control of Leprosy,” Boston Med. and Surg. Jour.,
Oct. 25, 1894, and Morrow, “Prophylaxis and Control of Leprosy in this Country,”
Trans. Amer. Derm. Assoc. for 1909; and Dyer, “The Sociological Aspects of Leprosy
and the Question of Segregation,” Jour. Cutan. Dis., 1911, p. 268, and discussion
(Brinckerhoff, C. J. White, Schamberg, Pusey, Morrow, and G. H. Fox), ibid., p. 282.
3 See papers and discussions in Trans. Internat. Leprosy Conference for full details
of the claims and experimental trials of the various special remedies.
936 NEW GROWTHS
even of small quantities. As less irritating to the stomach, the active
principle of the oil, gynocardic acid, has been also commended, usually
in the form of magnesium or sodium gynocardate, in the beginning dose
of ½ grain (0.033), and increasing gradually to 3 grains (0.2) three times
daily. Unna1 makes a soap of the oil with soda, and gives this coated
in pill form, and states that, according to his observations so far made,
in this method of administration there is no disturbing influence on di
gestion. Conjointly with the internal administration it can also be
prescribed by inunction. For this purpose it is mixed with 5 to 15 parts
of olive or cocoanut oil, or as a 50 per cent, ointment with lard. It is to
be rubbed in thoroughly, and, when possible, one to two hours daily.
Before each fresh application the skin is washed with soap and water
or by means of a warm bath.2 Under the favorable influence of this drug
the various disease manifestations abate, sometimes slightly, in others,
but relatively few, quite decidedly, and exceptionally the malady is
halted in its progress.
Gurjun oil (gurjun balsam, wood-oil, from the Dipterocarpus tur-
binatus) has had the warm support of Dougall, Hillis, and some others.
It is usually administered in emulsion, composed of 3 to 5 parts of lime-
water to 1 of the oil, and of which the dose is 2 to 4 drams (8.-16.) two
or three times daily. It is also usually to be conjointly prescribed by
inunction, with 1 to 3 parts of lime-water or olive oil, and thoroughly
rubbed in one to two hours daily. Strychnin, or nux vomica (formerly
as Hoàng nàn, powdered bark of Strychnos gaultheriana), is another
remedy which has had considerable reputation. It is frequently pre
scribed with one of the above oils. Piffard and G. H. Fox, of our own
country, observed in one or two instances practical recovery under their
conjoint use. Morrow also speaks well of the action of this drug. These
three remedies, together with others which may be demanded by general
indications, supported by hygienic measures, frequent baths, good food,
open-air life, and, when possible, change of climate, will often accomplish
much toward at least retarding the progress of the malady.
Many other remedies or plans of treatment have been variously
tried or advocated, more especially in recent years. Unna has spoken
well of ichthyol internally conjointly with external applications of re
ducing agents, to be again referred to. Sodium salicylate and salol
have also had favorable mention, and arsenic has long been considered
of possible value. Although mercury has been more or less considered
as detrimental in the disease, lately Haslund and Crocker have reported
markedly beneficial influence in several instances, the drug being ad
ministered by hypodermic injection deeply into the muscular tissue.
Crocker employed the perchlorid of mercury, using ¼ grain (0.016) in
20 minims (1.33) of distilled water twice weekly. Carreau, and also
Dyer, believe that good effects are sometimes obtainable by increasing
doses of potassium chlorate, an observation previously made by Chis-
1 Unna, Monatschefte, 1900, vol. xxx, p. 139.
2 Tourtoulin Bey, Monatshefte, 1905, vol. xl, p. 88, commends the administration of
the oil by subcutaneous injections, preferably into the subcutaneous tissues of the fore
arm or leg—dosage, 75 minims (5.).
LEPRA 937
holm. Montesant1 and Wellman2 have reported favorable influence
from salvarsan intravenously administered. Wilkinson3 reports a few
apparent cures from x-ray treatment. In recent years various attempts
have been made with treatment with serum (Carrasquilla), antivenene,
or attenuated snake poison (Calmette, Dyer, Woodson), tuberculin
(Yamamoto), and various vaccines—leprolin, nastin, etc (Rost, Deycke,
Rost and Williams, Wise, Minnett, Gottheil, Whitmore, Clegg, Duval
and Gurd, and others), but while at times favorable influences were
noted, the results have been, as a whole, as yet disappointing.4
The external treatment consists essentially in the maintenance of
cleanliness and an aseptic condition of the general surface, in order, so
far as possible, to avoid the suppurative complications due to infection
by pyogenic cocci. Frequent baths, the use of boric acid, formalin,
carbolic acid, and resorcin lotions, and sometimes sulphur baths, are
some of the measures to this end. Certain remedies have, however,
been employed with alleged special influence, such as Chaulmoogra
and gurjun oils, already mentioned, the inunctions of which, in addition,
however, have in view absorption and some constitutional action.
Cashew-nut oil has been similarly employed, both externally and inter
nally. In the opinion of some the good effects of these oils externally
1Montesant, München. Med. Wochenschr., 1910, No. 9, and 1911, No. 11.
2 Wellman, Jour. Amer. Med. Assoc, Nov. 16, 1912.
3 Wilkinson, “Leprosy in the Philippines with an Account of its Treatment with
the X-rays,” Jour. Amer. Med. Assoc, Feb. 3, 1906.
4 “Carrasquilla Serum,” discussion, Trans. Internat. Leprosy Congress, Berlin, 1897.
“Antivenene,” Dyer, ibid., vol. iii, p. 500, and New Orleans Med. and Surg. Jour.,
Oct., 1897, and Woodson, Philada. Med. Jour., Dec 23, 1899.
“Tuberculin,” latest report by Yamamoto, Japanische Zeitschr. f. Dermalologie und
Urol., Aug., 1912—abs. in Jour. Cutan. Dis., 1912,p. 739—treated a series of 30 cases
with old tuberculin, with alleged remarkable improvement in many.
“Leprolin,” Rost, Indian Med. Gaz., May, June, and Dec, 1904, made from the
culture of the bacillus; Rutherford, Indian Med. Gaz., Feb. 1913, p. 61, 32 cases treated
with leprolin, 20 followed throughout, questionable results, while taking it more deteri
orated than improved.
“Nastin, B.” Deycke, Lepra, 1907, p. 174, made from culture of a streptothrix
found by him in a nodular leprosy, from which he extracted a neutral fat which he called
nastin; this he combined with benzol chlorid in oily solution and called it nastin B.;
this latter is usually employed, nastin sometimes giving rise to alarming reaction;
Brinckerhoff and Wayson, “Studies in Leprosy, U. S. Gov. Printing Office,” 1909—6
cases, disappointing; Wise, Jour. London, Trop. School of Med., 1911, p. 63,—abs. in
Brit. Jour. Derm., 1912, p. 82—in 118 cases of various degrees “nastin” treatment
seemed only successful in 3 cases, the results approximating recovery; 70 patients were
placed on an injection of benzol chlorid in mineral oil (the nastin process without
the nastin), and the results as a whole were rather better than with the nastin; Wise
and Minnett, Jour. Trop. Med., Sept. 2, 1912, p. 259, summary of 244 cases treated
with nastin, at first thought to be encouraging, but proved at the most only a slight
temporary check; Gottheil, Jour. Cutan. Dis., 1911, p. 239, 1 case, some improvement.
Editorial review, Indian Med. Gaz., Feb., 1913, p. 71, regarding nastin treatment, by
Harris, Megraw, and Barnardo, states action doubtful.
Other vaccines: Whitmore and Clegg, Philippine Jour. Sci., Dec, 1910, p. 559,
treatment with glycerin extract and soap solution made from vaccine which Clegg had
cultivated from an acid-fast bacillus from the spleen and from the nodules from a num
ber of leprosy cases—results negative; nastin B. in 17 cases negative; Rost, Indian
Med. Gaz., July, 1911, vaccine prepared from cultivation of the leprosy streptothrix,
reports 5 of 12 cases treated as symptomatically cured—injected weekly 1 c.c. of a 1:
400 dilution of dried culture or the equivalent thereof and 1 c.c. of a sterilized six weeks
broth culture; Rost and Williams (loc. cit.), vaccine prepared from a culture of leper
bacillus in a medium consisting of distilled volatile alkaloid of rotten fish, lenco broth
(without salt or peptone), and milk; obtained hopeful results.
938 NEW GROWTHS
used lie, in great part, in the associated prolonged rubbing. Unna has
strongly commended, along with the internal administration of ichthyol,
the local applications of ointments containing the reducing agents,
resorcin, pyrogallol, chrysarobin, salicylic acid, and also ichthyol; a
compound formula recently advised by him, consisting of salicylic acid,
2 parts; ichthyol and chrysarobin, each, 5 parts; vaselin, 100 parts.
To limited areas the pyrogallol can be added in the same quantity as the
chrysarobin, or can be substituted for the latter. In some instances
excision and curetting of the nodules and infiltrations have been practised,
but the results are scarcely such to justify such heroic measures. Ulcera-
tions should be kept thoroughly cleansed, and, so far as possible, aseptic,
by the use of hydrogen dioxid washings, weak corrosive sublimate solu
tions, boric acid lotions, and similar applications. As ointments for apply
ing to open lesions may be mentioned those containing aristol, resorcin,
salicylic acid, ichthyol, balsam of Peru, and the like. Robertson1 com
mends applications of formalin, using it diluted to open wounds and pure
to other lesions. For the relief of the painful neuralgias, sometimes
of severe character, Rake and others have reported good results from
nerve-stretching. Electricity has been employed with some benefit
to anesthetic areas.
1 Robertson, Jour. Trop. Med., 1904, p. 26.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |