| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
GRANULOMA FUNGOIDES1
Synonyms.—Mycosis fungoides; Granuloma sarcomatodes; Inflammatory fungoid
neoplasm; Fibroma fungoides; Lymphodermia perniciosa; Sarcomatosis generalis;
Fr., Lymphadénie cutanée; Mycosis fongoide; Ger., Multiple Granulationsgeschwülste;
Mycosis fungoides.
Definition.—A chronic malignant disease characterized usually
by percursory symptoms of months' or years’ duration, of an eczematous,
1 Literature, usually with review and bibliography, and together, with the other
literature referred to in the course of the text, covering the entire subject: Duhring,
Arch. Derm., 1879, P.1, and 1880, p. 1 (with 2 case illustrations and 3 histologic cuts;
autopsy); De Amicis, “Dermo-linfoadenoma fungoide,” Naples, 1882, and Trans,
Internat. Med. Cong., Washington, 1887, p. 275; Vidal and Brocq, La France medicale,
1885, pp. 946, 957, 969, 983, 993, 1005, and 1018; Tilden, Boston Med. and Surg. Jour.,
1885 (with colored plates and histologic cuts), 2, p. 386; Payne, Trans. London Patholog.
Soc'y, 1886, p. 22, and “Rare Diseases of the Skin,” 1889; Ledermann, Archiv, 1889,
vol. xxi, p. 683, with 2 cuts, review, and bibliography; Pélissier, “Mycosis fongoide ou
Lymphadénie cutanée,” These de Montpellier, 1889—abs. Brit. Jour. Derm., 1890, p.
56; Besnier, Jour. mal. cutan., 1892, p. 314; Annales, 1892, p. 241; Funk (loc. cit.);
Stelwagon and Hatch, Jour. Cutan. Dis., 1892, pp. 1 and 51 (with colored plates);
Besnier and Hallopeau, Annales, 1892, p. 987; Morrow, Jour. Cutan. Dis., 1896, p.
465 (with colored plate and other illustrations); Hyde and Montgomery, ibid., 1899,
p. 253 (the last three papers deal more especially with the “premycosic” stage); Gal
loway and Macleod, Brit. Jour. Derm., 1900, pp. 153 and 187 (with 4 histologic cuts);
Joseph, Archiv, Ergänzungsband, 1900 (Kaposi’s Festschrift), with illustration and his-
tologic cuts; Stowers, Brit. Jour. Derm., 1903, p. 47, reports a case, and gives a table of
31 cases (and résumé of 20 of them) reported, published during the past ten years;
Riecke, Archiv, 1903, vol. lxvii, p. 193 (2 cases; 1, d’emblée type, died one-and-one half
years after onset; at autopsy metastatic growths were found in the kidneys, suprarenal
glands, retroperitoneal glands, and dura mater); Sereni, Dermatolog. Zeitschr., 1904,
p. 41 (girl of sixteen, a mycosis d’emblée, death two and one-half years from onset);
Greig, Brit. Jour. Derm., 1904, p. 251 (histologic report by Macleod); Hancock, Jour.
Amer. Med. Assoc, 1904, vol. xlii, p. 705 (case report, with autopsy and histologic
findings); Bozzi, Policlin (Rome), 1904, vol. xi, p. 97; Hodara, Monatshefte, 1904, vol.
xxxviii, p. 490 (3 cases treated by ichthyol internally, with improvement), in 2
cases investigated found at beginning of the malady a characteristic leukocytosis;
Pelegatti (mycosis fungoides and leukemia), ibid., vol. xxxix, pp. 369 and 433; Towle,
Boston Med. and Surg. Jour., 1904, vol. cli, p. 629; Schiele, Petersb. med. Wochenschr.,
1904, vol. xxix, p. 535; Ullmann, Monatshefte, 1904, vol. xxxix, p. 631 (chiefly histologic);
Orton and Locke, Jour. Amer. Med. Assoc, Jan. 12, 1907 (2 fatal cases; pathologic
GRANULOMA FUNGOIDES
905
urticarial, or erysipelatòus aspect, with the subsequent appearance of
pinkish or reddish, tubercular, nodular, lobulated, or furrowed tumors
or flat infiltrations, which frequently ulcerate and form fungoidal or
mushroom-like growths.
Alibert was the first to call attention to this rare affection, although
he originally thought it allied to yaws and described it (1814) as “pian
fongoide,” but afterward (1832) gave it the name of mycosis fongoi’de,
on account of its mushroom-like tumors. Among other later writers
who have added contributions to the subject may be mentioned Besnier,
Vidal, and Brocq, in France; Duhring, Morrow, Hyde, Tilden, Blanc, and
myself, in this country: Payne, Galloway, and Macleod, in England;
Auspitz, Geber, Köbner, Kaposi, and Schiff, in Germany and Austria;
and De Amicis, in Italy.
Symptoms.—As ordinarily observed, the course of the disease
may be divided roughly into several stages: The first stage is that of
erythematous and slight eczematoid manifestations, comprising, as a
rule, fugacious erythematous lesions, such as simple erythema, mild
erythematous eczema, and urticarial efflorescences; the second stage
(stage of infiltration) is somewhat similar to the first, except that the
eruptive phenomena show a degree of infiltration and are not so evanes
cent in character. The third stage is distinguished by its tumor growths,
varying in size from a pea to an orange, with a disposition to become
superficially ulcerated and fungoidal; but even these lesions may appear
and disappear more or less capriciously. The next stage is that in which
the ulcerations tend to become deeper-seated, with a marked fungoidal
tendency, and we then have the disease presenting itself as a conglomera
tion of eczematoid eruption, tumors, fungoid masses, mushroom-like
or crateriform ulcers. Exceptionally, the first two stages, which may
be considered the premycosic, may be extremely short or entirely want
ing. In most instances, however, the first, or earliest premycosic stage,
is an ill-defined one, with symptoms, often those of eczematous appear
ance, patchy or diffused, and usually with remissions or even temporary
periods of freedom. Intermingled with the erythematous or erythem-
atosquamous eruption there may be at times some urticarial or hive-
like efflorescences, and rarely there may be noted, independently or con
jointly with the other manifestations, some papular or even vesicular
findings, and brief review with references); Giovannini, Archiv, 1906, vol. 1xxviii, p.
3 (1 case associated with universal alopecia; 2 plates); von Zumbusch (of Riehl’s clinic),
Archiv, 1906, vol. 1xxviii, pp. 21 and 263 (5 cases; clinical, histologic, blood, and treat
ment); Roman, Jour. Cutan. Dis., 1910, p. 506 (2 cases; autopsy in 1 case, numerous
lesions in lungs, and apparently involvement of stomach, and marked enlargement of
lymph-glands; in second case x-ray treatment seemed to bring about toxæmia); Pardee
and Zeit, Jour. Cutan. Dis., 1911, p. 7 (case woman aged 57; pathologic findings of the
tumors of the skin, and internal organs suggest a true lymphatic leukaemia, but the
clinical picture was that of granuloma fungoides, at least indistinguishable from the
latter. This valuable contribution is largely illustrated (case and histologic illustra
tions, including histologic cuts of liver and lung); Strobel and Hazen, “Mycosis Fun-
goides in the Negro,” Jour. Cutan. Dis., 1911, p. 147, 2 cases; illustrations; a study
and review; analytic tables of data and bibliography of the disease and various allied
diseases; C. J. White, Boston Medical and Surgical Jour., May 4, 1911 (case report, fe
male aged 46, death, after seven or eight years; pyonephrosis (left); autopsy, new
growth-like mass in peritoneal cavity, histologically similar to that of the corium of
the skin).
906
NEW GROWTHS
lesions of an eczematous character, and exceptionally an eruption of a
psoriatic aspect.1 Very rarely the earliest lesions may be papular.
Probably the most frequent early or primary manifestation is an ery-
thematosquamous plaque, usually circinate or well defined, one or several
inches in diameter, which may be present scantily or in numbers. In 1
of my cases there was primarily a single plaque of this character at the
axillary fold, which lasted over a year, and then under treatment dis
appeared, to be followed a few months later by the appearance of several
scattered patches. This insidious beginning is not uncommon, and the
possibility of the earliest area being the point of infection—if the malady
can be so considered—is a matter of considerable interest and import.
The eruption may, and usually does, become quite extensive, and to all
appearances consists of ill-defined, circumscribed and diffused, reddened
areas, with often slight scaliness, and, as a rule, but little, if any, per
ceptible infiltration. The red color of the eruption is often slightly
mellowed by a yellowish tinge.
After thus continuing for months or several years or more, the second
stage—the stage of infiltration—is gradually presented. This infiltra
tion is more especially noted with the circumscribed areas. Soon small
pea- to cherry-sized, rounded or flattened nodules begin to appear,
scantily or in profusion. These, as well as the diffused erythematous
patches, may disappear suddenly, to be supplanted by similar lesions on
the same or other regions. The color of the eruption at this time is, as
a rule, a duller red than in the earliest period, and the red may at times,
or in places, have a violaceous or brownish hue.
Sooner or later the next or tumor period is imperceptibly ushered
in. The infiltrated patches or nodules become more infiltrated and larger,
and lead to the formation of distinct tumors; or these latter arise from
apparently normal surface; at first they may be few in number, the
earlier cutaneous phenomena still playing the chief rôle. They are of
different sizes, from a cherry to an egg, and exceptionally approaching
the size of an orange. As a rule, however, the earliest tumors are small,
not usually exceeding the size of a hen’s egg. They are solid in charac
ter, with rounded or oval configuration, and generally come slowly.
They frequently disappear, but others continue to come, ordinarily much
more thickly and larger and larger, although they may be present in
scant number throughout. In isolated growths, the largest, as a rule,
there are sometimes noticed softening and ulceration at the apex. The
disease progresses, the tumors are noted to be larger, and show a greater
disposition to break down, and the last stage of the disease is entered—
the fungoidal stage and what might also be called the cachectic stage.
In the previous period the general health seems unaffected, except as to
the depression produced by the knowledge of the existence of the malady
and the loss of sleep which may result from the itching. In fact, this
1 In the case reported by Biddle (The Physician and Surgeon, Jan., 1900) the earlier
eruption resembled psoriasis, the body being profusely covered with a brownish-red,
slightly elevated, scaly eruption, of a variegated pattern, but with a tendency to irreg-
lar oval and gyrate figures. In one of Strobel and Hazen’s cases (loc. cit.) the primary
lesions were papules, usually seated at the follicular openings, and often with either a
normal or broken hair piercing the center.
Plate XXIX.
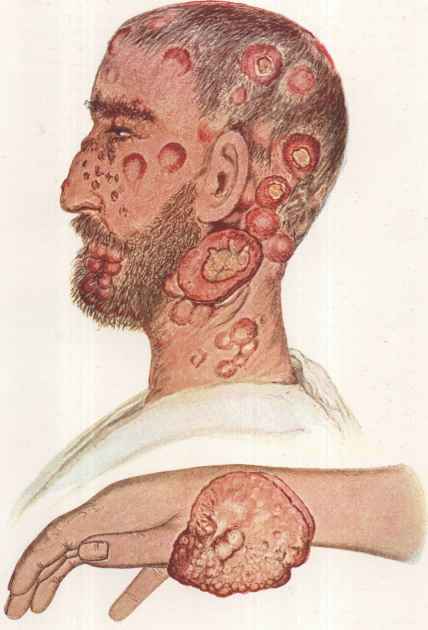
Granuloma fungoides. Case shown in the upper illustration was of thirteen years'
duration, the tumor stage being present the last fifteen months; the black-and-white
text-cut (Fig. 227) is of this same patient. The case shown in the lower illustration was
in a woman, the eczematoid symptoms and the tumor growths presenting about the same
time, death following a year after their first appearance. (These cases are reported in full
in Jour. Cutan. Dis., 1892.)
GRANULOMA FUNGOIDES
907
tempestuousness of the skin disturbance and practical absence of con
stitutional involvement until a late stage is, in most cases, the most
striking characteristic of this strange and essentially fatal malady.
This involvement may, indeed, not take place until the latter end of the
fungoidal ulcerating stage.
This period has as its special feature the ulcerating tumors; these
are frequently numerous, and result from the previously developed
growths, which are usually somewhat flattened on top, especially the
largest, the surface softening and ulceration extending from the central
apex portion almost to the edges. In some cases, however, as in one
reported by Whitfield,1 the eczematoid symptoms continue to be predomi
nant, with but a scanty admixture of ulcerating fungoidal tumors.
Some of the tumors may be somewhat pedunculated, the basal portion
being slightly or markedly smaller in diameter than the surface and pro
jecting part. The destructive tendency extends somewhat into the
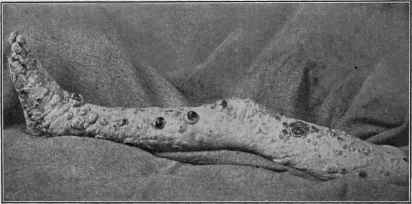
Fig. 227.—Granuloma fungoides in a male aged forty-seven, of thirteen years’ duration.
growth, but not always uniformly, and in such instances there results
a mushroom-like, ulcerating tumor, sometimes with everted edges, or
one the surface of which presents a resemblance to the surface of a cut
tomato, and with a mucoserous or purulent discharge, often mixed
with blood. The disease thus continues, the patient becomes weaker
and weaker, and distinctly cachectic, with symptoms common to sep-
ticemia, and which lead more or less rapidly to death.
Exceptionally the precursory or premycosic stages are entirely lacking,
and the disease first shows itself by the appearance of the peculiar fun-
goidal tumors, which are, as a rule, few in number, and usually limited
to one region—mycosis d’emblée, of the French. In this variety the
eczematoid and erythematous symptoms are sometimes subsequently
added. The lymphatic glandular system may or may not show special
involvement, although in most of the cases enlargement has been noted.
The course of the malady is usually slow, except in those cases in which
1 Whitfield, Brit. Jour. Derm., 1898, p. 153 (with 2 illustrations).
908
NEW GROWTHS
active fungoidal ulcers present at once; the duration before the final
end varies within considerable limits from several months (Galliard,
Naether, and Debove) to fifteen years or more; in one of my patients
thirteen years.
Etiology.—The cause of the disease is not known.1 The litera
ture discloses that it is much more common in males than females; ac
cording to Tilden’s analysis of 30 cases, 23 of the former to 7 of the latter.
In 4 cases under my own observation 3 were males and 1 female. It is
an affection of middle adult life, most common between the ages of forty
and fifty. In over half of Tilden’s tabulated cases it began after forty,
and in one-fourth under thirty, but no case before the age of twenty.
Demange’s patient (quoted by Tilden) was aged sixty-eight. It occurs
apparently among all nationalities, is entirely independent of syphilis,
tuberculosis, and leprosy, and with no evidence of heredity or contagion;
2 cases have never occurred in a family, and relatives and nurses fre
quently brought in contact with the patients have remained unaffected.
Micro-organisms (variously streptococci, diplococci, micrococci) have
been found and described by several or more investigators, notably
Auspitz, Rindfleish, Hochsinger and Schiff, Hammer, DeAmicis, Murray,
Hatch, and myself, but there has been no striking uniformity in the
findings; and others, as Kaposi, Payne, Dönitz and Lassar, Köbner,
Funk, Maiocchi, Vidal, Brocq, Tilden, Ledermann, and a few others
have either failed to find such organisms or, admitting their possible
presence, have looked upon them as either pyogenic streptococci or
merely fortuitous non-pathogenic forms. The inoculation experiments
made by Hatch and myself on 8 guinea-pigs and 8 rabbits were without
result.
Pathology.—There seems no longer doubt that granuloma
fungoides can scarcely be considered as belonging or allied to the true
sarcomata, as Kaposi, Funk, and some others believe; although there
are, as Bowen2 and others have pointed out, many points of similarity,
both histologically and clinically, with multiple sarcomatosis of the pure
type. The fact that some of the growths may undergo involution is,
according to the dictum of Cohnheim, a proof of their non-sarcomatous
nature, but we know now that in some instances of sarcoma, especially
the multiple pigmented sarcoma of Kaposi, that such retrogressive
changes can also take place. The premycosic or, as Morrow prefers to
call it, the prefungoidal stage of granuloma fungoides, taken with the
whole clinical course, and to a less extent the histologic data, place it as
a distinct affection, although some of the cases of the disease in which the
tumor stage is ushered in at once would almost point to connecting or
intermediate examples. French observers are inclined to look upon
the disease as lymphadenomatous; the majority of German investiga
tors, led by Auspitz, Hochsinger, and Schiff, regard it as granuloma-
tous, and with this view the studies of Payne, Hatch, and myself
1 The case reported by McVeil, Murray, and Atkinson, Glasgow Hosp. Reps., 1898,
vol. 1, p. 53—full abs, in Brit. Jour. Derm., 1899, p. 69, in a farmer aged forty-three,
seemed to follow an injury on the temple due to a sheep kicking him while shearing it.
2 Bowen (‘‘Mycosis Fungoides and Sarcomatosis”), Jour. Cutan. Dis., 1897, p. 65
(2 cases).
GRANULOMA FUNGOIDES 909
are in accord. Paltauf1 is inclined to include the malady in the
class of anomalies of vegetation proposed by Kundrat, which com
prises pseudoleukemia and certain forms of lymphosarcoma. In this
connection it may be stated that in 3 instances (Biesiadecki, Philippert,
Kaposi) there was an associated leukemia. In the Pardee-Zeit Case
(loc. cit.) although the clinical picture was that of granuloma fungoides,
the pathological findings pointed to a true lymphatic leukemia. There
is no doubt, as Hyde and Montgomery state, that the premycosic erup
tions are not truly eczematoid, but are the initial manifestations and dis
tinctly a part of the disease itself. Hardy, Leredde, and others believe,
according to the same observers, even apart from the visible beginning
symptoms, that the apparently sound skin is also at this early period
the subject of characteristic pathologic changes. Excepting in a few
instances (Duhring, Gallaird, Riecke, Brandweiner, Lenoble, and White)2
neoplastic tissue has not been found elsewhere than in the cutaneous
and subcutaneous structures.
The various lesional formations, especially the tumors, have been his-
tologically studied by many observers (Kaposi, Payne, Paltauf, Fordyce,
Joseph, Hyde and Montgomery, Galloway and Macleod, Hatch, myself,
and many others), and agree in the main, but, as already stated, the inter
pretation placed upon such investigations has varied. In the exami
nations by the majority of observers the epidermis was found thinned,
the rete Malpighi a mere wavy line, the papillae squeezed out by the
pressure of the growth from below, making them shorter and broader,
and the corium infiltrated with small round cells. All likewise agree
in denominating the cells forming the tumors lymphoid, and many have
been able to distinguish a fine embryonal connective-tissue network.
The sections from the 2 cases, taken when living, investigated by my
self and Hatch, were taken from patches of skin approaching the normal,
from the simple erythematous locations, from the tumors of moderate
size, and form the fully developed growths. In the first, or almost
normal sections, a moderate round-cell infiltration was seen in the
corium, and the latter was also thinner than normal. In those of the
second were found turgescence of the capillaries, with a diapedesis of the
red blood-corpuscles and considerable round-cell infiltration, occurring
in spots; the epidermis normal, the papillae intact, the round-cell infiltra
tion being limited above by the rete Malpighi. In the section of tumors
of moderate size a most characteristic feature was the crowding together
of the lymphoid cells around the capillaries. In other respects they ex
hibited about the same structure as the larger growths, save that they
presented, in addition, some of the elements of the normal derm. In the
fully developed tumors the following presented: the field seemed to be
made up entirely of lymphoid cells, having much the appearance of a
1 Paltauf (“Lymphatic Neoplasms of the Skin”), Vienna Congress, 1802 (quoted by
Bowen).
2 Duhring (loc. cit.) and Gallaird found neoplastic tissue in the walls of the bladder;
Riecke (loc. cit.) in the kidneys, suprarenal glands, retroperitoneal glands, and dura
mater; Brandweiner (Monatshefte, 1905, vol. xli, p. 415), nodular masses in both cere
bral hemispheres (colored illustration given), and Lenoble (Annales, 1908, p. 349) a
nodule in the right lung; C. J. White (loc. cit.) in peritoneal cavity.
910
NEW GROWTHS
small round-celled sarcoma, and reposing in a fine, embryonic, connective-
tissue stroma.
Diagnosis.—The recognition of the malady in the tumor stage is
rarely a matter of any difficulty, for the associated clinical symptoms,
usually present, of eczematoid eruptions, small and large nodules, and
walnut- to egg-sized or larger, elevated, ulcerating growths, generally
of a fungoidal character, and often one or several slightly pigmented
areas, showing the sites of tumors which have undergone involution,
taken together with the history, make up a picture which is unmistakable
and which also serve to distinguish it from sarcomata. In the variety
of granuloma fungoides in which the preliminary stages are wanting,
the tumors constituting the first signs, there may be strong clinical sugges
tions of sarcoma and carcinoma, but these latter usually show early
glandular involvement, are often spontaneously and acutely painful,
and rarely tend to fungoidal ulcerative forms, as do the growths in the
former malady. The diagnosis in the premycosic or prefungoid stages
is not always possible—indeed, in the earliest period wholly impossible,
as at that time the malady may show the clinical aspects of a mixed
urticarial, psoriasiform, and eczematous eruption, more usually, how
ever, eczematous in appearance. Inasmuch as Hebra once made the
diagnosis of eczema in a case, it can readily be seen that the symptoms
are sometimes clearly of this character in appearance, and that such an
error might be unavoidable. However, their persistence and capricious-
ness, the often circumscribed character of some of the areas, with no tend
ency to yield more than temporarily to therapeutic measures, and, in
the earliest stage, often a yellowish cast to the red, are features which
may lead to suspicion. To these later is added distinct infiltration,
usually of a more solid and well-defined nature than in eczematous or
psoriatic eruptions. Later still the small tumors appear, some of which
may lead rapidly to larger growths, and the difficulties in the diagnosis
disappear. In obscure cases a histologic examination of involved skin,
and even in the early phases of the disease, will usually show character
istic changes.1 Granuloma fungoides has also been confused with lep
rosy, but if necessary the examination for the lepra bacilli would serve
in the differentiation.
Prognosis and Treatment—The disease goes on to fatal
termination, the duration, as already stated, varying somewhat widely
from some months to fifteen years; after the active tumor stage is entered,
the patient can scarcely live more than some months or one or two years
at the most, depending principally upon the number of the growths and
the degree of ulcerative tendency displayed2 A case of recovery after
an accidental migrating erysipelas was recorded by Bazin, one after the
1 Gaucher, Joltrain and Brin, “Soc de Biologie, Sèance,” Nov. 6, 1909; and de
Beurmann and Verdun, Bull, de Soc. fran. de Derm, et Syph., 1909, p. 397, claim that a
serum reaction test similar to the Wassermann using an alcoholic extract of the mycosis
tumors as the antigen is of valuable diagnostic aid.
2 Elliot (discussion), Jour. Cutan. Dis., 1910, p. 682, refers to a case, seen by him
in 1892; of three years’ duration, in the erythematous stage with some tumors; patient
still alive and well, after eighteen years, although there had been returns of the tumors,
and the erythematous condition persisted to a certain extent; growths were burned
out with Paquelin’s cautery as soon as they appeared.
LEUKEMIA CUTIS; PSEUDOLEUKEMIA CUTIS 9II
administration of arsenic by Köbner, and one by Geber. Constitutional
treatment consists essentially in the use of tonics and nutritives, together
with the continued administration of arsenic, hypodermically, when
possible. Treatment by exposure to x-rays,1 using care not to have the
current too strong or the exposures too long, may often be resorted to
with benefit;2 even cures, as a rule, but temporary, however, have re
sulted. Instead of using one tube, and treating part after part separately,
Lawrence employs an x-ray bath, employing 6 tubes at the one exposure.
The treatment seems especially valuable in controlling the pruritus.
Results in some cases occurred without distinct x-ray reaction; in others
not till moderate reaction was provoked. Crocker cites a case in which
recovery took place apparently from continued purgation. Hodara
saw improvement from ichthyol, internally, moderate to full doses.
Local measures have in view the maintenance of cleanliness. In the
early stages the various antipruritic applications used in eczema can be
employed. Later, antiseptic applications and dressings to the ulcers,
and, when deemed advisable, operative interference.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |