| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
1162 PARASITIC AFFECTIONS
BLASTOMYCOSIS
Synonyms.—Blastomycetic dermatitis; Saccharomycosis hominis; Dermatitis
blastomycotica; Oidiomycosis of the skin; Fr., Blastomycose cutanée; Ger., Hefenmy-
kose; Hautblastomykose.
It is especially to the studies primarily of Gilchrist, and later of
Hyde, Hektoen, Bevan, F. H. Montgomery, and Ricketts, that the ex
istence of this cutaneous malady has been made known.1 It begins, as
1 Gilchrist, Johns Hopkins Hospital Reports, 1896, vol. i, p. 269; Hyde, Hektoen,
and Bevan, Brit. Jour. Derm., 1899, p. 261; F. H. Montgomery and Ricketts, Jour.
Cutan. Dis., 1901, p. 26; Hyde and Ricketts, ibid., p. 44 (with analytic table and
references); Stelwagon, Amer. Jour. Med. Sci., Feb., 1901; and Ricketts, Jour. Med.
Research, Dec, 1901. This last by Ricketts, which is largely based upon the work and
case reports by Hyde and F. H. Montgomery, with their photographs and photomicro
graphs, gives a presentation of the literature and a résumé of the published cases of
Hessler, Wells-Senn, Brayton, Anthony-Herzog, Dyer, and others to date; F. H. Mont
gomery, Jour. Cutan. Dis., 1902, p. 195 (2 cases).
Later literature: F. H. Montgomery, Jour. Amer. Med. Assoc., June 7, 1902 (cases
of Hyde and Montgomery; finely illustrated); Busch, Bibliotheca Medica, 1902, vol. ii,
part 10 (illustrations and bibliog.); “Second Annual Report of the Cancer Committee to
the Surgical Dept. of the Harvard Med. School,” Jour. Med. Research, 1902, vol. vii,
No. 3; Gilchrist, Brit. Med. Jour., 1902, vol. ii, p. 1321 (negro; with illustrations,
review, and bibliography); Sheldon, Jour. Amer. Med. Assoc, 1902, vol. ii, p. 1356;
Walker and F. H. Montgomery, Jour. Amer. Med. Assoc, April 5, 1902 (death from
systemic infection); Dyer, American Medicine, Oct. 25, 1902; Sequeira, Brit. Jour.
Derm., 1903, p. 121; Pusey, Jour. Cutan. Dis., 1903, p. 223 (2 case demonstrations,
with illustration); McCarrison, Indian Med. Gaz., April, 1903; Löwenbach and Op-
penheim, Archiv, 1904, vol. lxix, p. 121 (3 plates); F. H. Montgomery, Jour. Cutan.
Dis., 1903, p. 19 (followed by systemic tuberculosis and death); Ormsby and Miller,
Jour. Cutan. Dis., 1903, p. 121 (illustrations; cutaneous and systemic case; death;
autopsy); Evans, Jour. Amer. Med. Assoc, June 27, 1903 (infection was introduced
through a punctured wound inflicted while performing an autopsy on a patient that had
died of systemic blastomycosis); Shepherd, Jour. Cutan. Dis., 1902, p. 158; H. R.
Varney, Detroit Med. Jour., 1903-4, vol. iii, p. 73; Fischkin, Chicago Med. Recorder,
1903, p. 408; Wright, Northwest. Lancet, 1904, p. 149; Dubreuilh, Jour, de méd. de
Bordeaux, 1904, p. 529, and Annales, 1904, p. 865 (first French case); Unna, Munch,
med. Wochenschr., 1904, p. 1367; Clary, Medicine, 1904, p. 818; Koehler and Hall,
Jour. Cutan. Dis., 1904, p. 581 (in a negro); Eisendrath and Ormsby, Jour. Amer.
Med. Assoc, 1905, vol. xlv, p. 1045 (case with systemic involvement, illustrated; with
a review of the previously reported cases of generalized infection); Christensen and
Hektoen, ibid., 1906, vol. xlvii, p. 247 (2 cases, generalized); Bowen, Jour. Cutan.
Dis., 1906, p. 30 (case demonstration); and Bowen and Wolbach, Jour. Med. Research,
1906, p. 167 (first Boston case); Sakurane, Archiv, 1906, vol. lxxviii, p. 211 (probable
case—first Japan case; with case illustrations); Bevan, Jour. Amer. Med. Assoc, Nov.
11, 1905 (copper sulphate treatment); Primrose, Edinburgh Med. Jour., Sept., 1906,
p. 215 (Toronto case; lived there since aged fen, except two years spent in Chicago,
1897-1900; disease developed early, 1901); Kessler, “Blastomycosis in an Infant,”
Jour. Amer. Med. Assoc, 1907, vol. xlix, p. 550 (with good illustrations. Child five
months old; face and scalp); Herrick, “Generalized Blastomycosis: Report of a Case
with Recovery,” Jour Amer. Med. Assoc, 1907, vol. xlix, p. 328; L. Hektoen, “Sys
temic Blastomycosis and Coccidioidal Granuloma,” Jour. Amer. Med. Assoc, 1907, vol.
xlix, p. 1071 (review and references; believes these two allied but distinct); A. W.
Brayton, “Blastomycosis and Its Congeners: Report of Eight Cases Observed by the
Writer in Indiana,” Trans. Indiana State Med. Assoc, 1907-8; F. H. Montgomery,
“Systemic Blastomycosis; Autopsy and Successful Animal Inoculations,” Jour. Cutan.
Dis., 1907, p. 393 (with case, culture, and histologic illustrations); Shields, “Two
Cases, One Becoming Systemic with Fatal Termination,” Jour. Cutan. Dis., 1909, p.
156 (illustrations of 1 case); Ormsby, “Cases of Bromid Eruption Mistaken for
Blastomycosis,” Jour. Cutan. Dis., 1909, p. 445; Hutchins, Jour. Cutan. Dis., 1908, p.
523 (2 cases, 1 a negro; in 1 case, left lower lid and contiguous tissue; negro case illus
trated, disease involving eyelids, face, and back of left hand); Fontaine, Haase, and
Mitchell, “Systemic Blastomycosis: Report of a Case,” Archives Int. Med., Aug., 1909
(with excellent photomicrographs of sections of liver and lung showing organisms);
Washburn, “Systemic Blastomycosis,” Jour. Amer. Med. Assoc, April 15, 1911 (ex
ternal lesions mostly of abscess character; death; necropsy showed lung involvement);
Plate XXXIII.
Blastomycosis dermatitis. The black-and-white text-cut (Fig. 307) shows the same
case at a later period, partly healed on the back of the hand, but extending further on the
fingers and with a new centre on the wrist.
BLASTOMYCOSIS
1163
a rule, as a small, pea-sized papule or papulopustule, which slowly, in the
course of days or several weeks, has enlarged to the diameter of a dime, flat
tening down centrally and showing crusting. Upon removal of the crust
the surface is noted to be irregular and somewhat papillomatous, with
occasionally, at this stage, and almost always later, a variable amount
of seropurulent fluid between the papillary projections. The border
of the patch is elevated, reddish, usually of a deep red tinge, and well
defined by moderate infiltration. Either by increase peripherally, as
well as sometimes with the arising of new foci just outside the border, the
area covered may in several months or a year or so be considerable in
extent. The enlargement may occur in all directions or preponderantly
on one side, or it may be somewhat linear in extension. When at all
developed the malady consists of an elevated, irregular, papillomatous

Fig. 307.—Blastomycosis; man aged forty-nine; duration four years; healing tendency
in central portions.
area, of a deep-red or florid color, and with a moderate or tolerably free
seropurulent secretion. In places, especially the oldest parts, partial
or complete healing may take place, the surface skinning over and ex
hibiting a thin, atrophic, or scar-like appearance. There is but little
tendency to actual ulcerative action. Exceptionally, as in one of my
cases, foci of disease present some distance off, as, for example, up the
arm when the back of the hand is the site, and may assume the same
features or present as a small, flattened, sluggish, carbuncle-like for
mation, breaking at several points and discharging; in some respects
resembling sporotrichosis. In many cases in its gross features it is
Posey, Carpenter, and Allen J. Smith, “Peculiar Blastomycetoid Organisms Met in
Two Cases of Parasitic Conjunctivitis,” Univ. Pa. Med. Bull., Nov., 1908; Shepherd
and Rhea, “A Fatal Case of Blastomycosis,” Jour. Cutan. Dis., Nov., 1911, p. 588 (case
illustration and histologic cuts; blastomycosis of skin, bones, peritoneum, lymph-nodes,
pleura and lungs, kidneys, left adrenal, prostate, and esophagus).
1164 PARASITIC AFFECTIONS
almost a clinical counterpart of tuberculosis verrucosa. In other
cases the clinical aspects are closely analogous to those of lupus vul-
garis. The general health, except in the comparatively uncommon
cases of systemic infection,1 does not seem to suffer; in the latter
instances the general symptoms are such as are usually seen in tu
berculous and septic conditions, terminating sooner or later in most
such cases in a fatal outcome. On the other hand the disease may be
purely a local affair, and be even limited to a very small area—in one
instance reported to the nail region,2 in another to the tongue,3 and in
the case herein pictured to one ear.
Etiology and Pathology.—The malady is rare, and in about
75 per cent, of the cases is seen in men, and for the most part in those
over forty. The family history has shown no special tendency or vul
nerability. The investigations have disclosed the presence of the yeast
fungus as the causative agent. In a few instances the disease started at
the point of a slight abrasion or traumatism. The back of the hand,
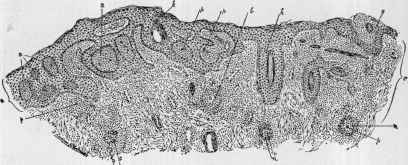
Fig. 308.—Blastomycosis, showing hypertrophied epidermis (e), numerous miliary
abscesses (a), which contain parasitic organisms (p). In the corium (c) are miliary
abscesses (b), pseudotubercles (n), with giant-cells (g) and parasites (p) (courtesy of Dr.
T. C. Gilchrist).
face, and lower part of the leg are the favorite localities. A blastomy-
cetic infection on other skin diseases is a possibility.
The histopathologic characters are in a measure similar to those
found in tuberculosis verrucosa cutis. These findings, as shown by
the investigations of Gilchrist, Hyde, Hektoen, F. H. Montgomery,
Ricketts, and others, are succinctly expressed by Ricketts: “Naked-
eye inspection of a cross-section shows, from without inward: (1) A
papillary zone, composed of a superficial layer of isolated villiform proc-
1 F. H. Montgomery and Ormsby, “Systemic Blastomycosis: Its Etiologic, Patho
logic, and Clinical Features, as Established by a Critical Survey and Summary of
Twenty-two Cases—Seven Previously Unpublished; the Relation of Blastomycosis to
Coccidioidal Granuloma,” Archives Int. Med., Aug., 1908.
2 Selenew, “Onychia Blastomycotica, Ikonographia Dermatologica Fasc 3, plate
23,”—abs. in Jour. Cutan. Dis., 1910, p. 540 (mother and four children with nail condi
tions resembling trichophyton infection, due to blastomyces).
3 Capelli, Giom. ital., Sept. 23, 1912, p. 467—abs. in Jour. Cutan. Dis., Jan., 1913,
p. 51 (case of a woman presenting tumor consisting of six nodules on the back of the
tongue, which upon investigation and culture was proved to contain blastomyces;
guinea-pig experimental inoculation were confirmatory; the paper is illustrated).
BLASTOMYCOSIS 1165
esses, and a deeper layer of similar processes which are united side by
side. (2) A homogeneous, vascularized, grayish-red, cellular zone, in
which are formed minute abscesses. (3) An unaltered layer of subcuta
neous fat, as the limit of deep extension. . . . Stained sections
exhibit the following histologic features: (1) A vast amount of ‘carcino-
matoid’ epithelial hyperplasia. (2) Minute intra-epithelial abscesses.
(3) A granulomatous condition in the
corium, characterized by masses of plasma
cells, minute abscesses, and tuberculoid
nodules and giant-cells. (4) The presence
of a spheric, capsulated, budding organ
ism, particularly in the epidermal and sub-
epidermal abscesses, but also distributed
unevenly and in small numbers in epi
thelial masses and granulation tissue.”
The organism, or fungus—the blasto-
myces—is sometimes but scantily found.
It consists of a rounded, doubly con
toured, vacuolated body, averaging in size
10 to 12 µ. They are often seen in pairs,
and also as budding forms, but in the
tissues never exhibit threads, as observed
in cultures. Proliferation in the former
is by gemmation; it seems probable,
also, that endogenous spores may form
(Ricketts); Hyde and F. H. Montgomery
state that under certain conditions blastomyces multiply by sporula-
tion.1 The pathogenic rôle of the blastomyces has been shown by the
animal experimental inoculations recorded (Gilchrist and Stokes, Hyde
and Hektoen, F. H. Montgomery and Ricketts).

Fig. 309.—Blastomycosis—in
volving ear only.
1 It had been generally believed and conceded that the so-called protozoic disease of
Posadas, Wernicke, Rixford and Gilchrist, D. W. Montgomery, and others, Busse’s and
Curtis’ saccharomycosis hominis, and Gilchrist’s, Hyde and F. H. Montgomery’s blas-
tomycetic dermatitis, are practically expressions of the same disease proces; and that
the organisms isolated from the various cases differ in minor respects, but are so closely
related morphologically and biologically as to justify their inclusion in a common genus.
This still stands as the view of an increasing majority of observers; but dermatitis cocci-
dioides (D. W. Montgomery) as an independent malady has still some earnest advo
cates.
In later papers, D. W. Montgomery and his associates (see “Dermatitis Coccidi-
oides,” by D. W. Montgomery, Ryftsogel, and H. Morrow, Jour. Cutan. Dis., 1903, p.
5, with illustrations showing the organism; and “Dermatitis Coccidioides; Reasons for
Considering It an Independent Disease,” by D. W. Montgomery and H. Morrow, ibid.,
1904, p. 368) contend strongly against the view that the blastomycosis and the coccidial
cases are identical. Their principal differences stated are “that in dermatitis coccidioi-
des there is a great diversity in the clinical picture; the skin lesions, which resemble the
rottentomato-like lesions of the tuberous iodid of potassium eruption, may be scattered
widely over the skin, or occur as subcutaneous abscesses; the cutaneous lesions are fre
quently secondary to internal infection; it tends strongly to become generalized and end
fatally; the organism has a double cycle of growth without any feature in common, one
in the tissues, and one in culture media; the organism increases by endogenous spore-
formation, and budding has not been seen; in fresh specimens the double-contoured
sphere may often be seen to be surrounded by a halo of short filaments like the cilia of
ciliated epithelium; the organism is larger than blastomyces; the administration of po
tassium iodid has no control over the disease.” In discussing the last paper and the
1166 PARASITIC AFFECTIONS
Diagnosis.—The disease is to be distinguished from tubercu
losis verrucosa cutis, vegetating syphiloderm, lupus vulgaris, and
sporotrichosis. Its resemblance to the first is striking, but ordinarily
the border of the tuberculous eruption has a deeper, usually more viola
ceous, color, and is less apt to be extensive. Its usual method of begin
ning, course, and behavior are different from those of syphilis. The
latter is, moreover, more distinctly purulent, the discharge having a
greenish tinge and often an offensive odor. Lupus vulgaris is relatively
slow in its course, with often distinct ulcerative tendency, and frequently
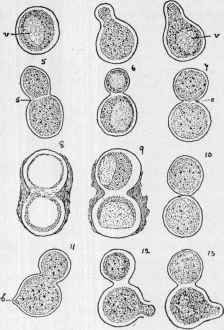
Fig. 310.—Blastomyces—fungus of blastomycosis. Nos. 2-13 represent various
budding forms found in the sections. Nos. 8 and 9 show the organisms with some form
of fibrous coating (courtesy of Dr. T. C. Gilchrist).
rather tough, firm scarring. The indolent abscess formation of sporotri-
chosis is more or less characteristic, and serves usually to differentiate.
conclusions, Gilchrist, Hyde, and F. H. Montgomery reiterated their already-known
changed views, accepting the identity of these various coccidial cases with those of
blastomycosis, citing cases of the latter which seemed to show phases similar to those
described by D. W. Montgomery. In the material from a case (Wright-Bolles case)
more recently examined by Wohlbach (“The Life Cycle of the Organism of Dermatitis
Coccidioides,” Jour. Cutan. Dis., 1905, p. 18) the organism found was identical with that
observed by D. W. Montgomery, Ryfkogel, and Morrow, and the writer also believes it
a distinct type; D. W. Montgomery, ibid., 1905, p. 115 (The Mould of Dermatitis
Coccidioides); Ophüls, Coccidioidal Granuloma (3 cases; with review of similar cases),
Jour. Amer. Med. Assoc, 1905, vol. xlv, p. 1291, and P. K. Brown, Coccidioidal Granu-
loma, ibid., March 2, 1907 (2 cases; with review), also agreed with these observers. See
also later paper, discussing this point from the negative side, by F. H. Montgomery
and Ormsby, Archiv Int. Med., Aug., 1908.
SPOROTRICHOSIS
1167
It is to be stated, however, that a positive conclusion in the differentia
tion with tuberculosis verrucosa, and to a less extent with lupus vulgaris
and with sporotrichosis, is possible only by microscopic examination,
cultures, or experimental animal inoculations.
The rare cases of the confluent papulopustular, papillomatous
eruption due to the ingestion of bromids and iodids present at times
a rough resemblance to blastomycosis. (See illustration under Dermatitis
medicamentosa.)
Prognosis and Treatment.—The ordinary verrucous type,
which remains distinctly cutaneous, is not dangerous to life, but it is
obstinate and sometimes destructive and distorting. The possibility
of systemic infection must be borne in mind, however, as the number
of such cases recorded is gradually increasing; they are always of serious
import.
Treatment, consisting of medication, x-ray, and excision or curet-
ing, is, as a rule, successful in the cutaneous cases. The iodids in
ternally in full dosage, with the maintenance of cleanliness and the
local use of weak iodin solutions or other antiseptic lotions, conjointly
with x-ray exposures (Bevan, Hyde and Montgomery, Ricketts, Shep
herd, and others), is the plan that most frequently brings about marked
improvement and sometimes cure. The iodids act slowly, however,
and must be continued for some months, the malady, in this respect,
differing materially from the vegetating syphiloderm, which usually re
sponds rapidly to the iodid treatment. Bevan has seen favorable
influence from ¼grain (.016) doses of copper sulphate, and the applica
tions of a 1 per cent, solution of the same drug. A persistent area or
remnant can be thoroughly cureted or excised. In systemic cases the
iodids should be pushed to extreme dosage, along with tonics and sup
porting measures.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |