| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
VERRUCA
Synonyms.—Wart; Fr., Verrue; Ger., Warze.
Definition.—Verruca, or wart, is a small, but somewhat vari
ously sized, circumscribed epidermal and papillary growth, which may
be soft or hard, and rounded, flat, acuminated, or filiform.
According to the shape and predominance of one of the several char
acters it is convenient to divide these formations into several clinical
varieties: verruca vulgaris, verruca digitata, verruca plana, verruca
filiformis, and verruca acuminata.
Verruca Vulgaris.—This is the common wart so frequently seen,
and occurring mostly upon the hands. It is somewhat variable as to
size, averaging that of a pea, and having a broad base. It is generally
hard or horny, somewhat rounded or slightly flattened, elevated, and
circumscribed. It is, as a rule, of slow and gradual growth, and at first
is smooth and covered with slightly thickened epidermis, but later the
smoothness usually disappears to a variable extent, and the surface
becomes, partly in consequence of the hypertrophy of the papillae, but
chiefly of the rete proliferation, rough and irregular, with minute ele
vations. Sometimes the projections are sufficiently pronounced as to
give it a slightly papillomatous appearance, and to give some cause
for the name “papilloma,” which has occasionally been used.1 In its
1The term “papilloma” was formerly used with a somewhat indefinite meaning
and indiscriminate application, not only to warts, but to all growths with projecting
excrescences or vegetations, which were then erroneously thought to be exclusively due
to papillary hypertrophy, and hence the name. Observation has shown that this fea
ture is only an accidental or occasional development, and, moreover, observed in various
and often totally diverse diseases, and is, therefore, not descriptive of any special
disease entity. For these reasons it is no longer to be considered a scientific term,
and has been practically dropped, and given place to the employment of the proper
disease title in each instance, with, to designate this particular clinical feature, the
addition of the descriptive adjective papillomatous, or its equivalent, papillary, vege
tating, verrucous, etc.—as, for example, the papillomatous or vegetating syphiloderm
(syphiloderma papillomatosa seu vegetans), papillary or papillomatous epithelioma,
lupus verrucosus, etc.
VERRUCA
547
earliest formation the color may be that of the normal skin, but later
it is grayish, with a slight or decided yellowish or brownish tinge; ex
ceptionally it is almost black. On the average there are several present,
but there may be but one, or they may be present in numbers. Not
uncommonly one lesion appears—the co-called “mother wart” (the
verrue mére of Vidal),1—attains full growth, and several others or more
gradually present, and usually close to the first or not far distant. Some
times several are in such proximity that coalescence ensues, and a wart
of relatively considerable size results. There are no subjective symptoms
—no itching,2 but, as with any other growths if irritated, they may be
come slightly painful when knocked.
While the fingers and hands are the usual sites of these lesions,
they are also occasionally found upon other parts, and Dubreuilh3 and
other writers4 have called attention to the fact that they are sometimes
observed on the feet, especially the soles (verruca plantaris, papilloma
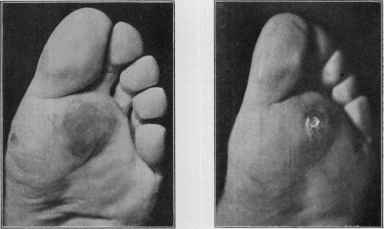
Fig. 129.—Plantar wart covered by cal- Fig. 130.—Plantar wart (same case)
lous, in a very frequent location (cour- after removal of the callous (courtesy
tesy of Dr. Richard L. Sutton). of Dr. Richard L. Sutton).
of the sole), where at times, from friction and pressure, the covering and
surrounding horny layer are much thickened, smooth, and hard, forming
a “wart-containing callosity,'’ so that they are usually mistaken for
corns; upon shaving off the surface the wart-like character is disclosed,
1 Vidal, “Verrue mére—verrues filles,” cited by Gémy, Annales, 1889, p. 94.
2 Corlett, Jour. Cutan. Dis., 1896, p. 301 (with illustration), reports a case of some
what doubtful nature in which numerous lesions of a warty character were on the legs,
and in which there was a good deal of itching; probably a case of prurigo nodularis
(q. v.).
3 Dubreuilh, “De la verrue plantaire,” Annales, 1895, p. 441; also review of this
paper by Bowen, Boston Med. and Surg. Jour., 1896, vol. cxxxv, p. 262.
4Eddowes, “Warts on the Feet,” Brit. Jour. Derm., 1896, p. 195; also “Corns,
True and So-called,” Brit. Med. Jour., Dec 21, 1895; D. W. Montgomery, Jour. Amer.
Med. Assoc, July 11, 1903; Berry, Jour. Cutan. Dis., 1904, p. 229; Bowen, Boston
Med. and Surg. Jour., 1907, vol, clvii, p. 781 (24 cases; histology; and ibid., vol. clxv,
p. 937; Sutton, Jour. Cutan. Dis., 1909, p. 155; and Amer. Jour. Med. Sci., July,
1912, p. 71 (with case illustrations).
548 HYPERTROPHIES
and in such operation bleeding is very readily produced. This plantar
wart is not an infrequent one in my experience, and is usually painful
and troublesome.1 The scalp may also be the seat of the common wart,
although in this region the digitate variety is the usual one. Excep
tionally the growths are found on the vermilion of the lips—on both lips
in a case observed by Elliot.2 In Gémy's3 case not only were the lesions
present in great numbers, but the legs were the principal seat.
Verruca plana, or the flat wart, is a name more especially used for
those pea- to finger-nail-sized growths, usually but slightly or moder
ately elevated, and observed most commonly on the back and face of
middle-aged and elderly people, although they may also occasionally
be seen in this form in younger individuals. In older people, however,
they are usually of a darker color, and not infrequently after a time be-

Fig.131.—Verruca of the juvenile flat variety in a young adult; was also on face and
forehead. There were some lesions, however, showing a tendency to develop into the
verruca vulgaris type.
come slightly papillomatous and covered with a rough, dark, often black
ish, somewhat greasy scale, constituting the formations also variously
known as keratosis pigmentosa, verruca senilis, seborrheic wart (verruca
seborrhœica), quite frequently seen associated with other degenerative
changes in the skin (see old age of the skin). There is sometimes slight
or moderate itching. They possess a close analogy at times to dark,
slightly elevated moles, and could be often clinically well described by
the term “warty mole.” There may be one, several, or more present,
and usually scattered. In some instances, sooner or later, there is a
tendency to development into epithelioma.
1 Hardaway and Allison, Jour. Cutan. Dis., 1906, p. 127, express the opinion that
these growths, as well as callosities, and hyperidrosis of this part are more common in
those having malpositions of the feet, especially flat-foot and Morton‘s foot.
2 Elliot, Jour. Cutan. Dis., 1889, p. 306 (case demonstration).
3 Gémy. “Verrues confluentes des deux jambes,” Annales, 1889, p. 94.
VERRUCA
549
Under verruca plana can also be most conveniently considered a
totally different variety of warts, both as to the age of those affected
and their clinical characters, known as verruca plana juvenilis, and
which has attracted notice in more recent years through the contribu
tions of Thin,1 Darier,2 Besnier,3 Herxheimer and Marx,4 and others.
Their sole feature possessed in common with the ordinary verruca plana
just described is the flat character, in other respects being wholly dis
similar. They are somewhat peculiar, lichen-planus-looking warts,
with roundish, squarish, or polygonal base, with a flat and smooth surface,
rarely larger than a small French pea, and usually much smaller, and
generally seated upon the face, where they may exist in moderate or
great number. Occasionally in some lesions a scarcely perceptible
central depression can be detected. They are normal skin color or gray
ish or brownish; are discrete or aggregated, and when several or more are
close together, coalescence sometimes takes place, resulting in a small,
irregular shaped, occasionally somewhat linear, patch. Their elevation
is usually slight, with some lesions scarcely appreciable. While all are
almost always perfectly flat, occasionally a few will show, especially in
their earliest existence, a slightly rounded top. The chin, lower part of
the cheeks, and the forehead, more particularly, as a rule, toward the
temporal region and the hair border, are the favorite situations. They
are seen in children, frequently in those quite young, but are also ob
served in youth and early adult age. They are generally slow and in
sidious in their coming, and are persistent, lasting often for months and
years, but unattended by subjective symptoms.
Verruca Digitata.—This is a variety of wart more commonly ob
served upon the scalp, and which is characterized by clefts or digitations
extending sometimes nearly or quite down to the base. This feature
may involve the whole body of the growth, but it is always most marked
at the peripheral portion. The wart may arise as such, being practically
of this nature almost from the start, or it may appear at first as an
ordinary wart, but as it grows, the epidermic covering seems to extend
down between the projecting and enlarging papillæ, while the latter
grow upward, and clefting results. When the digitations do not ex
tend completely to the base, the lower part, or neck, is sometimes
relatively much smaller or apparently constricted, and the growth has
then a pedunculated appearance, the upper cleft part tending to spread
out some. The surface is hard and horny, the lower portion somewhat
soft. If at all forcibly disturbed, they are apt to bleed—much more
readily than common warts. In size they vary from that of a small
pea to a dime, and are elevated from one to several lines. Their color
is usually that of other warts. But one or several may be present;
1 Thin, “An Unusual Case of Warty Growths on the Face,” London Med.-Chir.,
Soc'y Trans., 1881, vol. lxiv, p. 283 (with case illustration (colored plate) and two
histologic cuts).
2 Darier, “Verrues planes juveniles de la face,” Annales, 1889, P. 617.
3 Besnier-Doyon, French translation of Kaposi‘s work; also Annales, 1889, pp. 22
and 200 (in discussion).
4 Herxheimer and Marx, “Zur Kenntniss der Verrucæ planæ juveniles,” Münchener
med. Wochenschr., 1894, p. 591 (a report of 29 cases, with review of subject and refer
ences).
55O HYPERTROPHIES
quite frequently somewhat aggregated, sometimes sufficiently so to form
a coalescent group.
Verruca Filiformis.—This is a thread-like growth, most commonly
seated about the neck, face, and eyelids. It is of varying length, from
that of a line to \ of an inch or longer, and from scarcely more than a
thick thread to a line in diameter, apparently depending upon whether
one or several papillae are hypertrophied. It is, as a rule, soft to the touch
and quite flexible, with a narrowed conic or pointed end. It occurs more
frequently as a single formation, although occasionally several are to be
seen scattered or more or less closely grouped.
Verucca Acuminata (Synonyms: Condyloma acuminata; Venereal
wart; Moist wart; Pointed wart; Pointed condyloma; Condyloma acumi-
natum; Fig-wart; Cauliflower excrescence; Fr., Végétation dermique;
Ger., Spitzencondylom; Spitzenwarze; Venerische Papillome; Venerische
Warze; Feigwarze).—This variety usually occurs on the mucous and
mucocutaneous surfaces of the genital and anal regions, although also
sometimes on the adjoining integument and in the flexures and on other
parts.1 As they usually result from irritating discharges, they are most
common on the genitalia and genitocrural regions, and in association with
venereal diseases. The formations are either single or multiple, scanty
or abundant, pointed, tufted, club-shaped, and sessile or pedunculated.
They have a bright pinkish or reddish color, sometimes with a purplish
tone. In some cases they have the general features and color of a cock‘s-
comb. In other instances instead of projecting vegetations they have
more the appearance of thick hypertrophic and superabundant granula
tion tissue. In the mildest examples they consist of one or more groups
or bunches of acuminated, pinkish or reddish, raspberry-like elevations.
In extreme cases the warts make up irregular, cauliflower-like masses
which cover the entire region and project to considerable elevation.
According to the region, they may be somewhat dry or moist; and if
the latter, the secretion, which results from maceration due to the
natural heat and friction of the parts, is usually abundant, of a yellowish
color and puriform, and develops, from rapid decomposition, an offensive
and penetrating odor. As the excrescences bleed easily, the secretion
is sometimes tinged with blood. In some cases the discharge dries and
forms thickish, reddish-yellow or brownish crusts, sometimes tough and
almost horny, beneath which the partly pent-up secretion undergoes
rapid decomposition.
Their most common starting-points in the male are on the glans
and in the sulcus and from the inner side of the prepuce; and in the
female in about the clitoris, inner side of the labia, and from the vagina.
The anus may also be the site, and the condition may remain so limited,
but more commonly it appears here secondarily to the eruption on the
genitalia, especially in women. It may exceptionally also present upon
other regions, as about the axillæ, umbilicus, mouth, and between the
1 Heidingsfeld (Condyloma Acuminata Linguae), Jour. Cutan. Dis., 1901, p. 226
(with histologic cuts), reports an instance in which, in addition to lesions on the labia
majora, there were some similar warts on the tongue; and also reviews the subject of
extragenital verruca acuminata (with references).
VERRUCA
551
toes. On integumentary sites where there is not much or no friction or
excessive natural sweat secretion they are much drier, occasionally free
from discharge, and their color, at first at least, is not materially different
from the normal skin, but later becomes purplish and reddish. Their
development is commonly quite rapid, although sometimes, after attain
ing variable dimensions, they may remain more or less stationary.
In many cases, however, there is a disposition to increase and extend,
as the secretion is auto-inoculable. The malady is, in fact, contagious.
If undisturbed, there is usually no tendency to spontaneous disappearance.
Etiology.—Warts are more common in childhood, in adoles
cents, and in early adult life. There is a more or less general tacit
acceptance of mild contagiousness, and of the correctness of which I feel
pretty well convinced. Observations in many instances of suggestive
cases of auto-inoculation support such a view. The quite frequent
development of others from a primary or mother wart, to which Vidal
directed attention and which many others have noted, its spread by con
tiguity, as, for example, occasionally around the ungual borders, ob
served by Morrow, Allen, Bronson,1 and others, its spread from one
child or member to another of a family, as not infrequently observed, of
which Vivès2 recently reported an instance, are all suggestive. A short
time ago a gentleman was under my care with some warts on the hand,
who stated that his fiancée had also subsequently presented several
similar growths. Payne3 relates how in a case he thoughtlessly used
his own thumb-nail to scrape off a wart previously softened by an applica
tion, and that some time later a similar formation developed at this site
(under the edge of the nail), with subsequently two more on the thumb
higher up. These are a few examples to which many similar ones could
be added.
In fact, the clinical evidence is more than suggestive, and to this
we can now add the favorable inoculation experiments by Jadassohn,
Variot, Lanz, and one or two others.4 Lanz's experiment was con
vincing to him, although unsuccessful on the patient upon whom he
was experimenting; his patient had warts on one hand and forearm,
and a small portion of the growth was superficially implanted on the
arms, with negative result. He then tried rubbing across the large
or mother wart on the forearm on to the neighboring skin once or twice
daily for several days, using his first and second fingers, with no result
on the patient, but some time afterward three lesions developed on the
rubbing surface of his own fingers. The inoculations by the others
1 Morrow, Allen, Bronson, Jour. Cutan. Dis., 1899, p. 183 (case demonstration and
discussion).
2Vivès, “Verrues de Famille,” Jour. mal. cutan., 1899, p. 463 (3 members, one
after another).
3 Payne, “On the Contagiousness of Common Warts,” Brit. Jour. Derm., 1891,
p. 184.
4 Jadassohn, “Sind die Verrucæ Vulgares überträgbar?” Verhandl. der V. Deutschen
Dermatolog. Gesellsch. (1895), 1896, p. 497 (with review of the subject with references;
of 74 inoculations, made at different times, on 6 different persons, 31 were successful);
Variot, “Un cas l‘inoculation expérimentale des verrues de l‘enfant a l‘homme,”
Jour, de Clinique et de thérap. infant, 1894, No. 34, p. 529; Lanz, “Ein Beitrag zur
Frage der Ueberträgbarkeit von Warzen,” Correspondenzbl. f. Sshweizer Aerzte, 1898,
p. 264.
552 HYPERTROPHIES
named were on an extensive scale and seemingly conclusive. The incu
bation period is of long duration—from over one month up to seven or
eight, although probably, in favoring locations, as in Payne‘s case, a
much shorter period suffices. Jadassohn‘s experiments furthermore
apparently indicate, although not sufficiently positively, that the juvenile
flat wart produces its like, as does likewise an ordinary wart, and therefore
of different etiology. There is still wanting confirmatory proof of micro-
organisms, Kühnemann,11 believe, being the only one who has discovered
a microbe (a bacillus) of seeming pathogenic importance, and with which
he succeeded in producing suggestive lesions experimentally on rabbits.
The influence of slight traumatism, excoriations, pressure, and the like,
which were formerly considered as active causative factors, is now recog
nized as contributory toward furnishing favorable opportunities for suc
cessful inoculation. Schaal2 and others, however, are firm in the opinion
that local irritation—implantation of some minute foreign body, accord
ing to Schall—gives rise to hypertrophy of the connective tissue and pa
pillae, and thus produces the wart. Both Fox and Allen,3 and also myself,
have noted cases in which both molluscum contagiosum and warts were
present, and Fox is inclined to believe that there may be a common
cause or close connection. Such conclusion, it seems to me, is scarcely
warrantable when one considers the frequency of warts among the
poorer children, and with which cutaneous diseases other than molluscum
contagiosum could be found just as or more frequently associated, and
yet no question of relationship arise.
As to verruca acuminata, it is more than probable that this is an
entirely distinct affection etiologically from the other forms. With
these, irritating secretions are unquestionably of etiologic importance.
These warts and their secretions are doubtless contagious and auto-
inoculable. Ducrey and Oro4 found in the secretion, in the growth
and tissues, in addition to the staphylococcus pyogenes aureus and bacil
lus subtilis, two colonies of unknown micro-organisms, but experiments
with these latter on animals and man failed to produce any result.
Pathology.—From what has already been stated in discussing
etiology, it would seem highly probable that the initial factor in the
formation of a wart is a local irritation, and it is not unlikely that, in
most instances at least, this irritant is a microbic one. The organism
doubtless gains entrance, as Kühnemann suggests, through some small
break or fissure in the epidermis.
While anatomically (Bärensprung, Virchow, Auspitz, Unna, Kühne-
mann, and others)5 there are some slight differences in the several varie-
1 Kühnemann, “Zur Bacteriologie der Verruca Vulgaris,” Monatshefte, 1889, vol.
ix, p. 17; Schweninger stated (ibid., p. 380) that the culture-inoculations made by
Kühnemann had been apparently successful in rabbits.
2 Schaal, “Zur Aetiologie der Hautwarzen,” Archiv, 1896, vol. xxxv, p. 207 (the
accidental implantation of minute specks of glass gave rise to warts on his own hand).
3 Fox, Trans. Amer. Derm. Assoc. for 1888, p. 50 (discussion); Allen, “Molluscum
Contagiosum—an Analysis of 50 Cases,” Jour. Cutan. Dis., 1886, p. 238.
4 Ducrey and Oro (The Pathology of Condyloma Acuminatum), Naples, 1893—
abstract in Brit. Jour. Derm., 1894, p. 158.
5 Kühnemann, “Beiträge zur Anatomie und Histologie der Verruca vulgaris,”
Monatshefte, 1889, vol. viii, p. 341 (with two histologic plates, review of the subject,
and bibliography); Unna, Histopathology, p. 786.
VERRUCA
553
ties, there is primarily a connective-tissue growth or central prolongation
common to all, and the interior of which contains one or more vascular
loops; and to this are added varying degrees of epidermic and papillary
hypertrophy. In many the hypertrophy of the papillæ is more apparent
than real, due to their elongation and thinning by the epithelial growth;
in others there are fewer than normal, some being flattened down by the
proliferating rete. Both Auspitz and Unna, as well also as Kühnemann,
state the process starts in the rete and that the enlargement of the papillæ
is due, in fact, to the proliferation and downgrowth of the former, and
that the vascular and other changes in the corium are purely secondary.
The proliferation of the rete, which, as Kühnemann especially contends,
extends upward as well as downward, brings about some changes in the
upper epidermal layers, the horny layer in the ordinary wart being
usually markedly hypertrophied. Owing, however, to defective or
modified action in the process of keratinization, the thickened horny
layer is scarcely so dense or closely packed as normally, the nuclei,
according to Kühnemann, still being susceptible of staining. The his
tology of the peculiar small flat warts of children and young adults
(verruca plana juvenilis), according to the studies of Thin, Kühnemann,
Herxheimer, Jadassohn, Dubreuilh, and Darier, is, with the exception
of some minor differences, essentially that of the beginning verruca
vulgaris, although both Darier and Dubreuilh noted a slight preceding
exfoliation due to breakage and separation of the horny layers not ob
served in other warts.
The plantar wart has been studied histologically by Dubreuilh and
Bowen, with accord on the essential points. Bowen found no particular
deviation in the corium. The epidermis at the periphery showed pro
nounced acanthosis, papillary enlargement, down growth of the rete
plugs, and marked hyperkeratosis, together with great hyperplasia of
the granular cells; as the center is approached the middle rete cells
become vacuolated, appearing larger and rounder than their neighbors;
in many of the warts were seen peculiar protozoa-like bodies in many of
the nuclei of the rete cells, probably some form of nuclear degeneration.
The anatomy of the seborrheic wart—the verruca plana of old people
—has been studied by Neumann, Balzer, Handford, and Pollitzer,1
whose findings are somewhat divergent. Pollitzer's investigations are
the most recent and based upon material from 3 cases, and led to the
following conclusion: “The seborrheic wart is characterized histologically
by a slightly thickened stratum corneum, a considerably hypertrophied
rete, and in the papillary and subpapillary cells, the occurrence of epi-
thelioid cells arranged in groups and lines, separated by bundles of con
nective tissue, and teminating abruptly below the horizontal subpapillary
plexus of vessels; together with a peculiar infiltration of fat, affecting
the coil-gland epithelium, the middle and papillary layers of the cutis,
and epithelium of the rete; and perhaps an atrophy of the sebaceous
glands and hair-follicles.” The crust, more commonly found in those
1 Pollitzer, “The Seborrheic Wart,” Brit. Jour. Derm., 1890. p. 199 (with two his-
tologic cuts, and abstract of opinions of Neumann, Balzer, and Handford—with ref
erences.)
554 HYPERTROPHIES
who make little use of the bath, or more pronounced in such cases,
consists of fatty epidermic scales and foreign matter, wool-fibers, par
ticles of carbon, etc., often firmly attached and dipping down into the
follicles.
In verruca acuminata, made up largely of connective tissue ele
ments, are to be found marked papillary enlargement, excessive devel
opment of the rete, and an abundant vascular supply. The process
differs from the other warts in the absence of any special increase or
modification changes in keratinization (Unna, Kühnemann); in fact, the
horny layer is often almost or completely wanting. The most striking
and characteristic feature is the exuberant proliferation of the rete.
The connective tissue framework contains large blood-vessels and lym
phatics.
Diagnosis.—The characters of ordinary warts are so well known
and they are so unlike other lesions that a mistake can scarcely occur.
The somewhat rounded warts, with but little epidermic thickening,
might, in their beginning, be confused with the starting lesions of mol-
luscum contagiosum, but the central depression and aperture of the
latter, usually recognizable by the naked eye, certainly by a magnifying-
glass, would prevent mistakes; moreover, the face is their common site,
while verruca vulgaris is usually seated upon the hands. The plantar
wart differs from a callosity by its painfulness on pressure; by cutting
or shaving off the overlying callous the wart is readily recognized, and
it can thus be also distinguished from a corn, with which it is often con
founded. The small flat wart (verruca plana juvenilis) is suggestive
of lichen planus, but the latter rarely occurs on the face, except in very
generalized cases, and then to a relatively slight extent, whereas this is
the usual place for the small flat wart; and when the latter is also upon
the back of the hands and fingers, they are generally more numerous on
the face. Moreover, the lichen planus papules are usually larger, of a
darker, violaceous color, are itchy, and tend to run together and become
rough, scaly, and then show a good deal of infiltration, features not ob
served in small flat warts. Care should be taken not to confound this
juvenile flat wart, or the common wart, with the rare affections angiokera-
toma and xanthoma, more especially xanthoma multiplex and diabeti-
corum. The ordinary flat wart, or seborrheic wart, of advancing years
is usually upon the back, sometimes on the neck, and is, as a rule, quite
greasy or crusted, and of yellowish or blackish color, and can scarcely
be confounded with any other lesion. The raspberry or mushroom-like
character of verruca acuminata, and the localities affected, are sufficient
usually to prevent error with other lesions; they should not be confounded
with the flat moist papules of syphilis, which also occur about the same
parts.
Prognosis.—Warts, as commonly met with, have no significance
beyond disfigurement, being benign in character. The seborrheci
wart, as already stated, occasionally shows epitheliomatous develop
ment. This wart exhibits no tendency to disappearance; all the others
do, although they may last sometimes almost indefinitely. Verruca
acuminata, however, is usually persistent, unless measures are taken for
VERRUCA
555
its removal, although under the institution of rigorous cleanliness the
warts will frequently disappear without treatment. All these different
varieties are usually readily remediable, occasionally, especially the
plantar wart, requiring, however, persistent treatment, and sometimes
operative measures.
Treatment.1—The therapeutic management of verruca upon
which most reliance is to be placed consists of external treatment of an
antiseptic, caustic, or operative nature. It cannot be gainsaid, however,
that there is substantial evidence that a variable influence can be exerted
by certain remedies administered internally, more especially to be
advised in those instances in which numerous lesions are present. The
curative action of arsenic is well attested by the favorable experience
of a number of observers, among whom are Sympson,2 Pullin,3 Herxheimer
and Marx (loc. cit.), Thin (loc. cit.), Hallopeau and Leredde,4 and many
others. My own experience is confirmatory. It is to be given in mod
erate dosage, ¼ of a minim (0.016) or more to children, and 2 to 5 minims
(0.135-0.335) to adults, three times daily. In recent years magnesium
sulphate has been commended by Colrat,5 and its good effects in some
cases corroborated by Crocker,6 Brocq,7 and Hall,8 although many, nota
bly among whom Besnier and Bowen,9 have failed to see any influence.
The results were negative in several cases under my own care. It is
given three times a day, in dose of 1 to 20 grains (0.065-1.35) or so, ac
cording to age. Crocker (loc. cit.) states also that in some instances
full doses of nitromuriatic acid had seemed to be of service.
Whatever may be the differences of opinion as to the value of internal
medication, there is, of course, unanimity as to the effectiveness of local
treatment; and curious to say, that in occasional cases (among which sev
eral of my own)10 of more or less numerous lesions the removal of several is
followed by a spontaneous disappearance of the others.11 One of the best
methods of treating warts, more especially when but one or several are
1 Except when otherwise stated, the remarks apply to the several varieties, except
the seborrheic wart and verruca acuminata.
2 Sympson, “Note on the Treatment of Warts by the Internal Administration of
Arsenic,” Quarterly Med. Jour., 1893-94, vol. ii, p. 57.
3 Pullin, “The Treatment of Warts by the Internal Administration of Arsenic,”
Bristol Med. Jour., 1887, P- 269.
4 Hallopeau and Leredde, Dermatologie, 1900, p. 409.
5 Colrat, Lyon Médicate, 1886, vol. liii, p. 45 (soc‘y communication).
6 Crocker, Diseases of the Skin, third edit., p. 580.
7 Brocq, Traitement des Maladies de la Peau, second edit., p. 852.
8 Hall, Brit. Jour. Derm., 1904, p. 264. Both Watson (Brit. Jour. Derm., 1903,
p. 178), and Hall (ibid., 1906, p. 106) are inclined to believe that the purgative action
of this or other drug is the factor of importance.
9 Bowen, Twentieth Century Practice, vol. v (Diseases of the Skin), p. 637.
10 One of the most striking instances was a case in a male relative with 10 to 12
warts on each hand and which had been present for a year or more—removal with the
curved scissors of three of the largest (2 on one hand, 1 on the other) was followed in
the course of two to three weeks by spontaneous disappearance of all the others.
11 Galewsky (Ueber das spontane Verschwinden juveniles oder harter Warzen
an die Behandlung), Dermatolog. Wochenschr., 1912, liv, p. 589, had also recently re
ported such instances, and refers to similar experiences of other observers (Waelsch,
Barca), with references; Halberstaedter, Dermatolog. Wochenschr, Dec. 14, 1912, lv,
p. 1522, records on instances of disappearance (numerous warts on hands) after the
radiation of a small number of them; Delbanco, ibid., p. 1524, had a similar experi
ence, the warts on both hands disappearing after radiation of one hand.
556
HYPERTROPHIES
present, is by means of electrolysis, as originally suggested by Harda-
way. The growth is almost wholly or completely transfixed with the
needle attached to the negative cord, and the wet positive electrode
grasped by the hand or applied near by; the current is allowed to act
for thirty seconds to one or two minutes, according to the size of the
growth and the strength of the current—the latter varying from 1 to 4
or 5 milliampères. If the growth is hard, large, and old, the needle
should be withdrawn and reintroduced, crossing the first insertion. In
small lesions, and also in large growths, one to several introductions
from the top, instead of transfixing, will also usually be successful. The
wart either gradually shrivels away, or some irritation and crusting ensue,
which finally drops off, leaving occasionally a slight but scarcely per
ceptible scar. The method does not seem to be so satisfactory for warts
on the anterior aspect of the finger-bulbs, where they are usually sur
rounded with calloused and thickened epidermis, the operation here
sometimes producing considerable underlying irritation and swelling.
Various applications are also used and are often quickly effective;
paring, scraping, or sandpapering down of the lesion, except when the
epidermic thickening is insignificant, is usually a valuable preliminary.
I am in the habit, when the growths are at all numerous, of prescribing
frequently a saturated alcoholic solution of salicylic acid, with which
the warts are moistened once or twice daily, removing the softened warty
coating thus resulting from time to time. The same remedy is also often
used in collodion, 10 to 20 per cent. strength. If the latter is employed,
two or three coatings should be made night and morning for a few days,
and then, after the film loosens or cracks, as it commonly does in a day
or two, the parts are soaked in hot water, and the pellicle and softened
horny layer are rubbed off, sometimes using with advantage pumice
stone or scraping with a curet. The salicylic acid plan, which is, of
course, a mild one, is slow, and often not completely successful. Paring
or sandpapering the growth, combined with cauterization with silver
nitrate, and repeating every several days, is another mild, and often
efficient, though somewhat slow, method. Lactic acid applied scantily
one to several times daily also acts in some cases efficiently and without
much irritation, the softened surface being rubbed or scraped away from
time to time. Other applications resorted to are formalin,1 trichloracetic
acid, acid nitrate of mercury, and nitric acid; chromic acid, caustic
potash, and chlorid of zinc are also valuable, but are strong and destruct
ive and must be used with care. Carbon-dioxid snow (q. v.) has been
commended as a safe caustic. The application of the high-frequency
spark, by means of the carbon or glass-point electrode, has been lately
lauded.2 The constant wearing of a rubber covering—acting by its
macerating action—has also been commended.3
For the plantar corn-like wart I have usually employed the fol
lowing plan: the calloused covering is first removed by paring or by a
1 Engman, “The Nature of Some Epithelial Growths and Their Treatment with
Formalin,” Medical Review, 1900, vol. xli, p. 405.
2 Bulkley, Amer. Medicine, Nov. 19, 1904, p. 882.
3 Purdon, “Note on Verruca or Warts,” Dublin Jour. Med. Sci., 1899, vol. cviii, p.
99.
VERRUCA
557
few days’ application of salicylic acid plaster, or a 25 to 30 per cent,
ointment of salicylic acid continuously applied, and then the outer sur
face of the uncovered wart gently scraped or curetted away, or cau
tiously “melted away” with a strong solution of caustic potash, and
the cavity filled with salicylic acid and over this painted several coatings
of an 8 per cent, salicylated collodion; this must usually be repeated
one to three times at intervals of several days or a week. Bowen has
also had considerable success with salicylated collodion containing 10
per cent, of chrysarobin. The salicylated collodion plan alone would
doubtless cure most cases, if persisted in long enough, and especially
the strong salicylic ointment, removing the whitened horny layers from
time to time; this is also Bowen's belief, but, as he states, the necessary
patience is not found in all persons. Sutton commends highly the use of
carbon-dioxid snow, in pencil shape, applied firmly for 30 to 60 seconds,
then allowing tissues to thaw, and reapplymg, with slightly smaller pencil,
for 30 seconds, using boric acid powder as the after-treatment. Hard-
away and Allison believe the correction of any existing foot malposi
tion is helpful and sometimes curative.
The pedunculated and filiform warts can be readily snipped off with
the curved scissors, and the base touched with silver nitrate. This
method can also be used with the ordinary warts. I have found a good
plan in the scalp warts, usually the digitate variety, is gently to curet
and touch the base with pure carbolic acid or silver nitrate.
The small flat warts can be treated with repeated applications of
carbolic acid applied with a pointed match-stick or wooden toothpick,
or the milder applications already referred to can be employed. If
electrolysis is used, the needle is introduced superficially from the top,
and, as a rule, a mild current employed. In these cases, in which the
lesions are usually numerous and sometimes close together, I have seen
benefit from the use of a 5 to 10 per cent, sulphur or calomel ointment,
rubbed in in small quantity twice daily; also from a saturated solution
of boric acid with 2 to 10 or 15 grains (0.135-1.) of resorcin to the ounce
(32.) (Davis); and from Vleminckx's solution. Arsenic was at the same
time given internally.
The seborrheic wart is to be treated by frequent soap-and-water
washing and the rubbing in of a mild sulphur-salicylic acid ointment,
composed of 20 to 100 grains (1.35-6.65) of precipitated sulphur, 10
to 60 grains (0.65-4.) of salicylic acid, and 1 ounce (32.) of ointment
base, consisting of petrolatum or equal parts of petrolatum and lard.
If there is a thick or hardened horny layer or crust, the salicylic acid
collodion, already referred to, can be at first employed. Ordinarily
treatment well followed out can keep the growth down to clean plain
flat warts, and prevent the tendency to epitheliomatous degeneration
displayed in some lesions. If it is desired to remove the growth com
pletely, the stronger caustics named can be used, first, however, trying
the salicylic acid collodion, and a strong, 20 to 40 per cent, salicylic acid
plaster-mull or ointment. Trichloracetic acid sometimes acts satis
factorily. The carbon-dioxid snow is also valuable in these cases.
In the management of verruca acuminata the maintenance of cleanli-
558
HYPERTROPHIES
ness is absolutely essential. The parts should, therefore, be cleansed
at least twice daily by the ordinary washing methods, or, if numerous
and crowded, by free irrigation, and subsequently the bountiful use of
powdered boric acid, to which, in some instances, 1 to 10 per cent, of
alum can be added with advantage. Powdered alum alone is also some
times employed. A 5 to 10 per cent, solution of salicylic acid in equal
parts alcohol and water will prove curative in some instances. Painting
the parts with solution of subacetate of lead, pure or weakened, has also
been used. If these milder measures are unsuccessful, stronger remedies
must be resorted to, such as the careful application of glacial acetic acid
or chromic or nitric acid, tried in the order named.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |