| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
NAEVUS PIGMENTOSUS
Synonyms.—Pigmentary mole; Mole; Mother’s mark; Fr., Nævus pigmentaire;
Tache pigmentaire; Ger., Pigmentnævus; Fleckenmal; Pigmentmal; Linsenmal.
Definition.—Nævus pigmentosus, or mole, may be defined as a
circumscribed increase in the pigment of the skin, usually associated
with hypertrophy of one or all the cutaneous structures, especially of
the connective tissue and hair.
Symptoms.—Moles are of various kinds and degrees,1 and accord
ing to the predominance of one or other feature are divided into the
several varieties, nævus spilus, nævus pilosus, nævus verrucosus, and
nævus lipomatodes.
Nævus spilus is the simple pigmented smooth spot, consisting of a
pea- to bean-sized or much larger area, usually deeply colored from a
light brown to a black, and scarcely, if at all, elevated. Sometimes,
however, there is slight connective tissue increase with this, and when
so, the patch is slightly raised above the surrounding surface. One,
several, or more may be present. The face, neck, and back are favorite
situations. Nævus pilosus is the hairy mole, which in addition to the
features of the common smooth nævus, just described, presents an
abnormal growth of hair, slight or excessive, light in color or deeply
pigmented, and usually coarse and of considerable length. There is
often added a somewhat irregular surface and a variable connective-
tissue hypertrophy. They may be single or multiple, and may occur
upon any part of the body, and while ordinarily not larger than a bean,
may be of much greater area, and in extreme instances cover a portion
of or a complete region. The “bathing-trunk” or “bathing drawers/’
pigmented and hairy nævus, covering the region indicated by its name,
is an example of the extensive type.2
Nævus verrucosus, as the name signifies, is the mammillated or
warty pigmented nævus, with a rough, sometimes hard, sometimes soft,
irregular surface, and usually with variable, but often considerable,
increase of all the skin tissues, and with, often, marked hypertrophy of
the papillæ, this last feature giving rise to the furrowed and uneven
surface. There may be but slight development in the hair of the part,
but, as a rule, there is considerable growth. The nævus lipomatodes
is the type in which there is an excessive fat and connective-tissue hyper
trophy,3 producing sometimes formations of considerable dimensions and
1 The different forms are discussed in full, with bibliography, by Möller, Archiv,
1902, vol. lxii, pp. 55 and 371, and Riecke, ibid., 1903, vol. lxv, p. 65.
2 Howard Fox (Jour. Amer. Med. Assoc, April 20, 1912, p. 1190) records a typical
case and gives a brief review of 26 similar cases reported, with references; Dore
(Brit. Jour. Dem., 1912, p. 194, case demonstrated) also records a typical example
with illustration.
3 Jackson reports a good case, with illustration, in Jour. Cutan. Dis., 1895, p. 66.
516
HYPERTROPHJES
elevation, being soft and loose in texture, or somewhat verrucous and
hard, with or without hair hypertrophy. The surface is either smooth
or irregular and warty, and sometimes the growth shows loosely or closely
packed folds and deep furrows, occasionally having a mollusciform as
pect. As already stated the more common or ordinary moles are found
most frequently upon the face, neck, and upper part of the trunk,
although they may occur upon any part of the surface. The extensive
hairy, verrucous, and lipomatous moles sometimes cover a considerable
area, in extreme cases a great part of the trunk, and especially the lower
trunk and the ischiofemoral regions are partially or completely enveloped.1
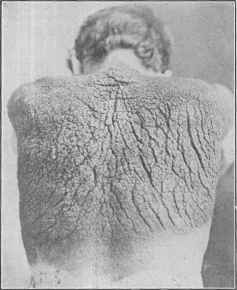
Fig. 122.—Nævus pigmentosus, congenital and of extensive distribution; except the
large irregular and clefted area on the back, they are nearly all small, smooth, and flat;
here and there, especially on those of the right shoulder and buttock, a growth of hair.
A slight secretion from the clefts of the large growth and of an offensive odor. This
growth has spread slightly during past few years, with the suggestion of possible ma
lignant change. Patient a Swede, aged twenty-one (courtesy of Dr. Burnside Foster).
While there is in most cases no special distribution or configuration,
in exceptional instances of apparently the same disease the lesions are
arranged in narrow bands, sometimes zosteriform, as in the De Amicis
and Hyde cases. These cases, usually limited to one side of the body,
have a peculiar form which has been described under the various names
of linear nævus, nævus unius lateralis, nævus nervosus, nævus lichenoide,
ichthyosis linearis neuropathica, papilloma lineare, papilloma neuro-
1 Remarkable cases, with illustrations, have been recorded in recent years by Michel-
son, Ziemssen‘s Handbook of Skin Diseases, p. 405; Hyde, Jour. Cutan. Dis., 1885, p.
193 (with references to other cases); Joseph, Lehrbuch der Hautkrankheiten, third edit.,
p. 181; Lesser (Baerensprung‘s case), Lehrbuch der Hautkrankheiten, tenth edit., pp.
234 and 235; Burnside Foster, Jour. Cutan. Dis., 1899, p. 132 (concerning the case
herein illustrated).
NÆVUS PIGMENTOSUS 517
pathicum unilaterale, etc.1 Cases vary to a slight degree, but only in
minor details, more especially as to extent, location, and width of the
band-like strips. The characters of the formation vary somewhat,
however, in different cases; most cases probably corresponding to a some
what hard nævus, with some accumulation of the horny layer, giving it
slight scaliness, and of a light or dark brownish color; or it may consist
of contiguous and distinctly small papillary growths. In other cases
the component lesions may be comparatively smooth and soft, with
variable pigmentation. Occasionally, as in the 3 cases, apparently of
this disease and of closely similar nature, reported by Thibiérge,2 Sel-
horst,3 and DaCosta,4 there is associated a comedo-like plugging of the
sebaceous ducts. In some cases, as in Morrow‘s, there is some itching.
Etiology and Pathology.—Moles are seen in both sexes, and
are usually congenital, sometimes being small and insignificant at birth,
and undergoing variable development later. Duhring and some others
believe that many of the flat, smooth, pigmentary nævi without hair,
which are seen so commonly upon the trunk, are not congenital, but
appear subsequently. Duhring states that they “are almost invariably
acquired during the life of the individual.” There is no doubt of this
in some instances according to my own observations, although it is
1A full list of the numerous names under which this peculiar form has been de
scribed is given in D. W. Montgomery‘s paper, “The Cause of the Streaks in Nævus
Linearis,” Jour. Cutan. Dis., 1901, p. 455 (with report of a case, with illustration).
Among the various case reports and contributions on this subject (linear nævus),
several with references and résumé of other cases, may be mentioned: Hyde, “Rare
Form of Congenital, Multiple, and Monolateral Pigmentary Nævus, Having the Dis
position of Zoster Corporis,” Chicago Med. Jour, and Exam., 1877, vol. xxxv, p. 377;
S. Mackenzie, “On Neuropathic Papillomata,” Illust. Med. News, 1888, vol. i, p. 123
(several cases with illustrations); Spietschka, “Ueber Sogenannte Nerven Nævi,”
Archiv, 1894, vol. xxvii, p. 27 (report of 3 cases, with illustrations, review of the sub
ject, and references); Werner and Jadassohn, “Zur Kenntniss der ‘systematisirten.
Nævi,’ " Ibid., 1895, vol. xxxiii, p. 341; and Jadassohn (second paper), “Bemerkungen
zur Histologie die systematisirten Nævi,” ibid., p. 355, and Jadassohn (third paper),
“Zur Localisation der systematisirten Nævi,” ibid., p. 373 (3 extremely valuable
papers and report of 9 cases, case illustrations, histologic cuts, and full résumé of the
disease, with bibliography).
Among other important papers: Hallopeau and Weil, Nœvi systématisés métamêr-
iques, 1897, p. 483 (with some references); Morrow, “Linear Nævus, with Remarks on
its Nature and Nomenclature (2 cases),” N. Y. Med. Jour., 1898, vol. lxvii,p. 1 (with
2 colored plates); Ransom, “An Unusual Case of Nævus Unius Lateris,” Jour. Cutan.
Dis., 1896, p. 141 (with case illustration, and histologic cut by Fordyce); Philippson,
“Ichthyosis cornea (hystrix) partialis, etc,” Monatshefte, 1890, vol. xi, p. 337 (2 cases
and 5 similar cases from literature—critically discussed; illustrations); Cutler, “Ich-
thyosis Linearis Neuropathica,” Jour. Cutan. Dis., 1890, p. 139 (case demonstration);
Peterson, “Ichthyosis Linearis Neuropathica,” ibid., p. 57 (with illustration and some
literature references); Müller, “Ein Fall von Nævus verrucosus unius lateris,” Archiv,
1892, vol. xxiv, p. 21 (with 2 illustrations); Colcott Fox, Brit. Jour. Derm., 1897,
p. 446 (case demonstration). Heidingsfeld, Jour. Amer. Med. Assoc, Aug. 27, 1904 (3
cases, with review and references); Hodara, Jour. Mal. Cutan., 1905, p. 61 (histologic,
with review and bibliography); Adamson (histologic), Brit. Jour. Derm., 1906, p.
235; Schalek, Jour. Cutan. Dis., 1908, p. 562 (case report, with illustration); Stowers,
Brit. Jour. Derm., 1908, p. 1 (a case, not unilateral, chiefly left side; several plates).
2 Thibiérge, “Nævus acnéique unilatéral en bandes et en plaques,” Annales, 1896,
p. 1298 (case demonstration).
3 Selhorst, “Nævus Acneiformis Unilateral is,” Brit. Jour. Derm., 1896, p. 419 (with
case illustration).
4 Mendes DaCosta, “A Case of Sebaceous Nævi”—abs. in Brit. Jour. Derm.,
1897, p. 207; original paper in Nederlandsch Tijdschrift voor Geneeskunde, Deel 1, No.
7, 1897.
518
HYPERTROPHIES
possible, as has been suggested, that there may have been previously
small, insignificant, unnoticed lesions from which their development
may have sprung. That a nævus may sometimes undergo variable
extension is a matter of observation, but much more commonly, however,
the only change in many instances is increase in the growth of hair.
Pathologically, an ordinary pigmented nævus is similar to a freckle,1
except that it is larger, and with usually, but not always, a variable,
though often slight, connective-tissue hypertrophy, and commonly
with the pigment extending more deeply; and with peculiar cells, usually
called “nævus cells,” suggestive of embryonic epithelium. The condi-
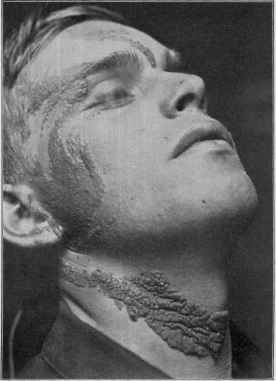
Fig. 123.—Linear nævus.
tions in the other forms vary: there may be hypertrophy of all parts of
the cutaneous structures, or a predominance of one or more over other
components. Their origin is somewhat obscure. Unna, speaking
jointly of angiomatous and pigmentary nævi, believes that they have a
hereditary basis or have their foundations laid in embryonic life, and
become evident at different periods later, developing slowly. This
1 Knowles’, (“Multiple Areas of Pigmentation,” etc, Jour. Cutan. Dis., 1912, p.
83, with review of similar cases and conditions, with case and histologic illustrations,
and bibliography) investigation would indicate that doubtless many of the thin,
superficial pigmented cases, heretofore considered as in the nævus class, really belong
pathologically to ephilis.
NÆVUS PIGMENTOSUS
519
practically corresponds to Kaposi's view, that they are the result of an
embryonic impulse in one or more of the tissues, which continues beyond
the usual normal limit. The cells of which a mole is chiefly composed
have generally been thought by pathologists, following Virchow‘s view,
to be of connective-tissue or endothelial origin, and their endothelial
origin has recently been maintained by Johnston,1 but Unna, Gilchrist,
Whitfield,2 and others have, in following out the histogenesis of these
growths, reached the conclusion that they are not of dermal, but of epi
dermal, origin. W. S. Fox,3 while largely sharing this latter opinion,
believes, from his investigations, there is also a rare variety of soft moles
whose cells are probably derived from the mesoblast.
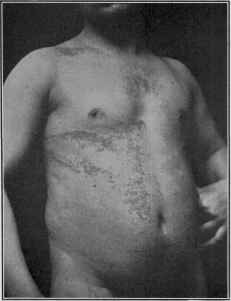
Fig. 124.—Linear nævus (lesions in this case were very much like those of lichen planus).
The position of linear nævus is somewhat problematic Unna con
siders that provisionally they might remain with the proliferative tumors.
Histologically, however, in the main, the characters are similar to those
of the other forms of nævi presenting like clinical features. Both Peter-
1 Johnston, “Melanoma,” Jour. Cutan. Dis., Jan. and Feb., 1905. (An elaborate
paper with numerous histologic cuts (two colored) and complete bibliography to date.)
Among others of the important recent papers on the pigmented moles are those of Fick
(included in Johnston‘s bibliography), Sachs, Archiv, 1903, vol. lxvi, p. 101 (with
bibliography), and Migliorini, ibid., 1904, vol. lxx, p. 413.
2 Gilchrist, Trans. Amer. Derm. Assoc. for 1898, p. 30; Writfield, Brit. Jour.
Derm., 1900, p. 268 (with bibliography and histologic cuts).
3 W. S. Fox, “Researches into the Origin and Structure of Moles and their Relation
to Malignancy,” Brit. Jour. Derm., 1906, pp. 1, 47, and 83 (with review and bibliog
raphy); Ziegler‘s investigations (“Beiträge zur pathologischen Anatomie und zur
allgemeinen Pathologie,” 19o6, vol. xxxix) show that in some instances the growth takes
its origin from the covering epithelium (“Deckepithelium”) and not from the nævus
cells themselves; Fich, “Ueber weiche Nævi,” Monatshefte, 1909, vol. iv, pp. 397 and
443, discusses the soft nævi at length, reviewing the literature in detail, with a full
bibliography.
520
HYPERTROPHIES
sen1 and Elliot2 found adenomatous involvement of the sweat-glands;
the latter, however, believing this finding to be an entirely secondary
and accidental one.
The origin of this linear nævus formation and distribution has been
the subject of much discussion. D. W. Montgomery‘s study of the
literature shows that the various theories advanced are: (1) The streak
or bands follow the course of the cutaneous nerves; (2) run along what
are called Voight‘s lines; (3) follow the lines of cleavage of the skin; (4)
follow the course of the blood-vessels; (5) run in the metameres or seg
ments of the body; (6) lie along the embryonic sutures and follow the
trend of growth of the tissues. The last, according to this writer,
more nearly explains the curious band distribution. Balzer and Alquier,3
in a recent study, conclude that the readiest explanation is upon the basis
of the Voight lines, and that the occasional divergence probably depends
upon embryonic malformation.
Prognosis.—Pigmentary nævi are permanent,4 but, as a rule,
when once established, do not tend to grow larger, although in many,
even of the ordinary, moles, later in life there is a disposition sometimes
noticed toward increased growth of the down or hair of the patch.
Beyond the disfigurement, however, the blemish is a benign one,
unless constantly irritated, under the influence of which, especially in
advancing years, degenerative changes set in and a malignant char
acter is occasionally noted. In some instances, it is true, apparently
without known irritation or traumatism, a nævus has been the starting-
point of more or less general malignant growths (see also Sarcoma),
as noted by several observers, among whom, most recently, Green,5
Gilchrist,6 and Waelsch.7
Treatment.—There are several methods of removing moles—by
electrolysis, caustics, and excision. Soft, pigmented fleshy moles,
those which have a peculiar tendency to lead to degeneration and
general carcinomatous (or sarcomatous) invasion, should be freely
excised, going well beyond the limits of the growth. Circumscribed
or even large hypertrophic moles can also be satisfactorily treated with
this method, but usually with variable disfigurement. Flat freckle-like
moles may also be removed satisfactorily with shaving over the skin,
just going deeply enough for the pigment—it is similar to the method
of procuring skin-graft.
1 Petersen, “Ein Fall von multiplen Knäueldrüsengeschwülsten unter dem Bilde
eines Nævus verrucosus lateris,” Archiv, 1892, vol. xxiv, p. 919.
2 Elliot, “Adeno-cystoma Intracanaliculaire Occurring in a Nævus Unius Lateris,”
Jour. Cutan. Dis., 1893, p. 168 (with histologic cuts).
3 Balzer and Alquier, “Les dermatoses linéares—Etude clinique et pathogenique,”
Arch. gén. de Med., 1901, vol. clxxxvii, p. 717 (19 illustrations).
4 Spitzer, Dermatolog. Zeitschr., 1905, p. 34, describes a case of verrucous nævus
which underwent spontaneous involution, and also refers to a similar one reported by
Lassar.
5 Ledham Green, “Ueber Nævi pigmentosi und deren Beziehung zum Melanosar-
com,” Virchow's Archiv, 1893, vol. cxxxiv, p. 331.
6 Gilchrist, “Are Malignant Growths Arising from Pigmented Moles of a Carcino-
matous or Sarcomatous Nature?” etc, loc. cit. (with histologic cuts and bibliography).
7 Waelsch, “Ueber die ausweichen Nævus, enstandenen bösartigen Geschwülste,”
Archiv, 1899, vol. xlix, p. 249 (with histologic cuts and bibliography).
ACANTHOSIS NIGRICANS 52I
In the ordinary surface non-hairy moles application of the “electric
needle” to several or more points, and but superficially inserted, not
going more deeply than the upper part of the corium, will sometimes
remove the blemish, especially after several repetitions, without leaving
much of a scar, and occasionally with scarcely any trace. With hairy
moles the hairs should be removed first by the ordinary electrolytic
method, and in some cases, when this is done, the pigment will have
almost completely disappeared, although, as a rule, supplementary
treatment, as just described, will be necessary. The elevated and ver-
rucous growths, if not too large, can also be treated in like manner, the
hairs, if present, being first removed. If the case is at all extensive,
this method is tedious, but much can be accomplished in the way of a
good result.1 The strength of current employed varies, according to
the character and nature of the growth, from one-half, in the superficial,
freckle-like lesions, to several or more milliampères in the thicker and
hypertrophic varieties.
In recent years, however, the favorite treatment for an average or
moderate case is by caustic refrigeration, as previously endorsed by Dade
and Trimble,2 and later by Pusey, Zeisler, Bunch, and many others,
including myself. Liquid air, originally employed for this purpose,
has given way to the easily procurable carbon-dioxid snow. The method
of using is described in the preliminary chapter on Treatment.
The superficial moles can also frequently be satisfactorily removed
by mild chemical caustics carefully and scantily used, such as trichlor-
acetic acid, glacial acetic acid, and nitric acid, applied by stippling or by
a thin coating to the surface; the deeper growths, by the same caustics
more energetically and repeatedly applied.
Linear nævus can in some instances be successfully treated by the
various methods described, but ordinarily the readiest plan is that by
excision. Ransom, in his case, after trying many methods, found
that the most satisfactory procedure consisted in picking the skin up
between the thumb and fingers, snipping off the top of the ridge thus
made by flat-pointed scissors, the cut being superficial and extending
not quite through the skin proper.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |