| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
ICHTHYOSIS 56l
ICHTHYOSIS
Synonyms.—Fish-skin disease; Xeroderma; Xeroderma ichthyoides; Ichthyosis
vera; Ichthyosis congenita; Sauriasis; Fr., Ichtyose; Ichthyose; Ger., Fischschuppen-
ausschlag.
Definition.—A chronic disease of the skin of congenital origin
or developing in early life, characterized by more or less generalized
dryness and harshness, slight to plate-like scaliness, and a variable
de gree of follicular papulation, sometimes warty or hornlike.
Symptoms.—Several grades of the disease are encountered,
but commonly classed under two heads—ichthyosis simplex and ich-
thyosis hystrix. The mildest
development of ichthyosis sim
plex is often referred to as xero-
derma (also xerosis), in which
the condition consists of scarcely
more than a dry, harsh, some
what rough-feeling skin, most
pronounced on the extensor sur
faces of the extremities, and on
the back, although commonly
recognizable also on other parts,
especially when the weather is
more or less continuously cold,
dry, and windy. There is usu
ally with this, or existing as the
predominant feature, a slight or
moderate degree of keratosis
pilaris, most pronounced and
frequently noticeable only on
its common situations, the an-
terolateral aspects of the thighs
and posterolateral surfaces of
the arms. There is generally
also branny scaliness, sometimes
more decided, and with a slight
tendency here and there to larger
thin scales, with a disposition
for the edges to turn outward
(general pityriasis). Not only is
the skin dry, harsh, rough, slightly
scaly, and often with a dirty-gray
ish or unwashed appearance, but
it is also somewhat lacking in sup
pleness and elasticity. There is a trifling thickening of the epidermis, and
usually a slight accentuation of the lines of the skin. The skin of such
patients is more susceptible to ordinary irritating influences, and in winter
exposed portions tend to chap readily, and commonly to show an ec-
zematous inclination.
36
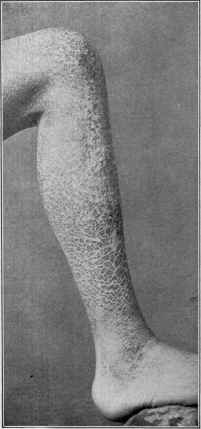
Fig. 134.—Ichthyosis of average develop
ment (courtesy of Dr. W. Frick).
562 HYPERTROPHIES
From this mild type there are many gradations to the extreme type
of ichthyosis simplex. In its slighter developments the scaliness is
more marked than described, consisting of thin, film-like, irregularly
shaped or quadrilateral scales, most striking about the extensor sur
faces of the region of the elbows and knees, but with, however, more
or less general slight development of keratosis pilaris than observed
in the mild form—xeroderma—just referred to. The face and scalp,
too, may show a slight dryness and furfuraceous scaliness. In more
marked cases all the features become exaggerated, the epiderm is con
siderably thickened, the scales are thicker and more plate-like, with
pronounced follicular keratosis and usually a universal involvement of
the surface, always most developed, however, on the surfaces named,
and in these cases the trunk as well often showing marked plate-like
scaliness. The plate-like scaliness gives the skin a fish-scale aspect,
and hence the name ichthyosis, or fish-skin disease. In still more
marked cases the scales are noted to be quite thick, plate-like, usu
ally more or less quadrilateral, divided by somewhat deep furrows;
and even the flexor surfaces of the joints—regions relatively or often
completely spared in the milder types—show slight or moderate involve
ment. The scalp is dry, scaly, and the hair often lusterless and lifeless-
looking, the face rough, dry, and covered with branny or film-like scali-
ness. The plate-like character of these extreme types is so strikingly
like the thick scales of certain fish or water animals, as the alligator,
as to give rise to the designation, “alligator skin.”1 In these, as well as
in some of the less developed examples, the elasticity and suppleness of
the skin are so compromised that mobility is more or less interfered with,
and fissures, often somewhat deep, occur about the joints. Moreover,
in these instances, as well as, in fact, in milder cases, during cold weather,
eczematous tendency and complication, especially of the face, hands,
and forearms, are usually observed, in which event the features of
this latter disease are superadded. Some subjects seem more predis
posed to the effects of irritation than others.2
These several grades represent examples of what might be termed
true ichthyosis, in contradistinction to ichthyosis hystrix, about the
status of which there is some difference of opinion. The condition of
the surface varies from a branny desquamation to that of thick, horny
plates, the latter usually more or less quadrilateral and roughly diamond
shaped. Those regions where the integument is thin and softer, as
the flexures, neck, face, inner part of the thighs, etc., are always less
involved than other parts, and in many of the milder cases are scarcely
or at all affected. The scales are exceptionally somewhat shiny and
seemingly translucent (ichthyosis nitida, ichthyosis nacrée), but usually
are dirty grayish, and, in marked and extreme cases, often brownish
gray, greenish, or blackish (ichthyosis nigricans). Other terms are
occasionally met with in literature—ichthyosis serpentina, or resembling
1 See papers by G. H. Fox, “The ‘Alligator Boy’—A Case of Ichthyosis” (with
colored plate), Jour. Cutan. Dis., 1884, p. 97; and by Yandell, “The ‘Man Fish’ of
Tennessee,” Louisville Med. News, 1878, p. 262.
2 Besnier, “Ichthyoses irritables,” Annales, 1889, p. 534.
ICHTHYOSIS
563
the skin of a serpent, ichthyosis sauroderma, or sauriasis, suggestive of
a crocodile skin, ichthyosis scutellata, scales somewhat shield shaped.
The hair and nails usually show nutritive changes, being harsh and lus-
terless, the nails being often quite fragile and easily broken. The sweat
and oil secretions are much dimin
ished, and sometimes in complete
or relatively complete abeyance.
As already remarked, there are
rarely any subjective symptoms,
occasionally slight itching, which,
however, is more commonly due
to eczematous complications. Fis
sures, when present, may however,
be quite painful.
The course of the malady in
these cases is usually quite char
acteristic, appearing early in life,
increasing slightly during childhood
and adolescence, and being less
pronounced during the warm sea
son and most marked in winter.
The type once established, whether
mild, moderate, or severe, remains
about the same throughout life.
In the milder cases, during the
summer weather, owing to the in
creased activity of the sweat and
sebaceous secretions, evidences of
the malady almost wholly or en
tirely disappear, to present again
on the approach of cooler weather.
In the severe types also there is a
variable lessening of the condition
during such period. The amount
of scaliness present in a given case
depends to some extent upon the
patient‘s habits as to the frequency
of general ablutions.
The malady is usually first noted in the first or second year, although
it is probably born with the individual, but that during the first months
it is so slight, the skin so frequently washed, and owing to the warmth
of the body, the consequently perspiratory action, favored by the usual
overclothing at that period, so free, that it could be thus kept in abey
ance, and its existence readily overlooked.1 In other rarer instances
1 Brocq and other French observers have in recent years called attention to a
form of ichthyosis (designated érythrodermie congénitale ichthyosiforme, congenital
ichthyosiform erythroderma) observed usually at birth, but which differs in some
respects from the ordinary cases of ichthyosis, more especially as to localization, in
the flexures, where it may be lichenoid; and with a shiny, reddened, varnished-looking
condition of the skin of the face, and wrinkled condition of the skin in general, with

Fig. 135.—Ichthyosis congenita. Case
photographed when four days old.
Mother pregnant seven times, giving
birth the fifth and the last (present case)
to infants with congenital ichthyosis; the
former (Sherwell‘s case referred to) still
living (courtesy of Dr. J. MacF. Win-
field).
564 HYPERTROPHIES
the child is born with all the conditions of a marked ichthyosis present,
sometimes of pronounced character (ichthyosis congenita, keratoma
diffusum, intra-uterine ichthyosis), examples of which have been reported
by a number of observers, among whom Lebert,1 Caspary,2 Hutchinson,3
Sutton,4 Elliot,5 Sherwell,6 Winfield,7 Schwartz,8 and others. The
scaliness in these cases varies from a brownish, parchment-like exfolia
tion to that of plate-like character, and usually with superficial or deep
rhagades, more or less ectropion, puckering and fissuring of the mouth
and other mucous outlets, and sometimes distortion of the nose and
ears as well, constituting the so-called “harlequin fetus.” These children
are, as a rule, prematurely born, and frequently do not survive many
days or weeks. Hebra and Kaposi have considered all these cases as
generalized seborrhea (ichthyosis sebacea), a view, however, which is
not at all in consonance with the observations of others.9 It is not im
probable that several maladies may present somewhat similar conditions
at birth, such, for instance, as a pronounced and somewhat persistent
vernix caseosa. Some of the milder cases presenting at birth a mem
branous coating somewhat suggestive of a layer of collodion or oiled
paper, such as those of Hallopeau,10 Grass and Törok,11 and Bowen,12
are, in the opinion of Bowen, “examples of a persistence of the epitrichial
layer, which has usually been cast off by the seventh fetal month, but
in these instances maintained its integrity up to the time of birth, when
it enveloped the infants like a distinct membrane, such as is found in
certain animals. After a short time this membrane begins to peel off
in large masses and sheets, leaving the normal skin below in a state of
moderate desquamation, which slowly subsides.” Grass and Törok
now and then a tendency to bleb formation, and to keratotic thickening of the palms,
or palmar aspects of the fingers, together with palmar and plantar hyperidrosis.
Jadassohn, Blatt fiir Schweizen Aerzte, 1911, No. 13, has more recently recorded 3
cases (demonstration); and Pernet, “Bullous Ichthyosis,” Brit. Jour. Derm., 1911,
p. 344, reports a case and gives a résumé of the French observations.
1 Lebert, Ueber Keratose, Breslau, 1864 (reviews 9 cases).
2 Caspary, “Ueber Ichthyosis Fœtalis,” Archiv, 1886, vol. xiii, p. 3 (2 cases, with
review and references, colored plate, and two histologic cuts).
3 Hutchinson, Clinical Lectures—Rare Diseases of the Skin, p. 172 (Mackenzie‘s
case).
4 Sutton, “A Case of Generalized Seborrhœa or ‘Harlequin’ Fœtus,” London Med.-
Chirurg. Trans., 1886, p. 291 (with colored plate, histologic cut, and bibliography).
5 Elliot, Jour. Cutan. Dis., 1891, p. 20 (2 cases, with review and some literature
references).
6 Sherwell, ibid., 1894, p. 385 (with some literature references).
7 Winfield, ibid., 1897, p. 516 (with case illustration and autopsy, and microscopic
examination by Van Cott). See also Wasmuth‘s recent paper, “Beitrag zur Lehre von
der Hyperkeratosis Congenita,” Ziegler's Beiträge, 1899, vol. xxvi, p. 19 (case illustra
tion, histologic cuts).
8 Schwartz, Bull, of Lying-in Hospital of New York, March, 1910, reports a case
with illustration: the mother had ichthyosis; her first child died at the age of 12 days,
with, according to the mother, the same malady (ichthyosis congenita) and also the
4th and 6th children (these two seen by Dr. Schwartz); the 4th child died on second
day after birth, the 6th child (the case pictured) died on the fourth day.
9 See Caspary and Elliot‘s papers.
10 Hallopeau and Watelet, Annales, 1895, p. 149 (case demonstration).
11 Grass and Törok, ibid., 1895, p. 104.
12 Bowen, “The Epitrichial Layer of the Epidermis and its Relationship to Ichthyo-
sis Congenita,” Jour. Cutan. Dis., 1895, p. 485 (gives abstract review of above two
papers); Meneau, “De l'ichthyose foetale dans ses rapports avec l‘ichthyose vulgaire”:
Annales, 1903, p. 97 (a thorough review with complete bibliography).
ICHTHYOSIS
565
take a somewhat similar view, but they would also include the ichthyosis
sebacea of Hebra and Kaposi in the same category. In the 3 cases
referred to “the general health was not visibly affected by the abnormality
of the skin.” A reading of the literature would indicate that, while
many, such as most of Lebert‘s, Elliot's, Sherwell's, Winfield‘s, and others,
are clearly examples of congenital or fetal ichthyosis, all reported cases
do not represent this malady—some the type of delayed physiologic
shedding just referred to, others doubtless generalized seborrhea (ich-
thyosis sebacea, persistent vernix caseosa), and, it is not improbable,
in a few instances, infantile dermatitis exfoliativa.
Ichthyosis hystrix is usually
looked upon, as already remarked,
as an infrequent variety of ich-
thyosis, but it has many features
which seem to stamp it as a prac
tically distinct affection. It is
rarely, if ever, generalized, but
usually limited to one or several
regions; exceptionally it is true,
it is more or less irregularly dif
fused. It presents in patches of
various size and shape, some
times ill defined, made up of
thickened, rough, warty-looking,
hypertrophic, papillary elevations
of variable size up to \ inch or
more. The surface is uneven,
more or less corrugated, some
times with horny, spinous growths,
which may be of considerable
dimensions—hence the term hys-
trix, or spiny, and also the term
applied to extreme cases—"por
cupine men” “hedgehog skin,'’
“rhinoceros skin.” In the milder cases of this type there is a resemblance
to the rough bark of a tree. The underlying skin is harsh, dry, and often
considerably thickened, and in some instances—suggestive connecting
cases between ichthyosis simplex and ichthyosis hystrix—the inter
vening surface is dry, rough, and scaly to a variable degree, corresponding
to that of the more common form of ichthyosis. As a rule, however,
the skin between or outside the areas is normal. In color the patches
vary somewhat, being yellowish-gray, yellowish, or greenish. Some
times the warty or spine-like protuberances are cast off from time to
time, as in one of the celebrated Lambert cases,1 to be rapidly repro
duced.
Limited and peculiarly shaped ichthyotic-looking eruptions, here-
1 Telesius, “Beschreibung und Abbildung der beiden sogenannte Stachelschwein-
Menschen aus der Englischen Familie Lambert,” oder “the Porcupine man,” Alten-
burg, 1802—abstract account by Lebert, loc. cit., p. 126.
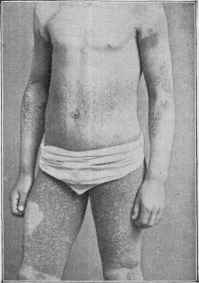
Fig. 136.—Ichthyosis hystrix in a lad
aged twelve, on parts below the knees of
mild (ichthyosis simplex) type.
566
HYPERTROPHIES
tofore included as cases of ichthyosis simplex and of ichthyosis hystrix,
such as “chronic palmar and plantar ichthyosis,” “linear ichthyosis,”
and “ichthyosis linguæ,” are no longer considered as belonging to this
malady. Chronic palmar and plantar ichthyosis corresponds to kera-
tosis palmaris et plantaris, linear ichthyosis to linear nævus, and ich-
thyosis linguæ ordinarily to leukoplakia. It is not improbable, more
over, that some cases of keratosis follicularis were formerly described
under ichthyosis. While ichthyosis simplex and ichthyosis hystrix
usually exhibit clinical distinctions throughout their course as to give
good ground for the belief in their individuality, yet in exceptional in
stances the features of both are seen to be present in the one case,—
constituting the mixed variety,—as in the case of my own here illustrated.
In this the hystrix variety of moderate degree is shown especially on
the thighs from the knees up, as well as less markedly in other places,
while on regions, as below the knees and elsewhere, the dryness, harsh
ness, slight to moderate scaliness, quite characteristic of ichthyosis
simplex. In Thibiérge's case,1 as in some others on record, the mixed
character was also observed. In this latter instance, moreover, the
mucous membrane of the mouth and nares shared in the process—an
extremely rare and almost unknown occurrence. Another exceptional
feature is an atrophic condition of the skin, which has been noted in a
few instances by Jadassohn,2 Hallopeau and Jeanselme,3 and Audry.4
Unusual features in a so usually well-marked malady as ichthyosis must
always be viewed with suspicion.5
Very rarely cases (described variously as ichthyosis follicularis,
ichthyosis cornea, pityriasis pilaris, follicular xeroderma, etc.) are met
with in which the brunt of the process seems to be predominantly follicu-
lar, presenting, clinically, features of a marked keratosis pilaris, and,
less strikingly, of keratosis follicularis, with a variable, underlying,
dry, xerodermic, or ichthyotic surface; in few such instances the malady
is not general. In some cases the projecting follicular spines, after fall
ing out, leave distinct atrophy; in others, involving the hairy regions,
there results more or less baldness. These cases are hard to classify.6
Etiology.—The malady is congenital, and in most cases a hered
itary tendency is noted, the history of one or more direct ancestors or
collateral relatives having the same disease being quite usual. While
the condition of the skin, referring more especially to ichthyosis simplex,
1 Thibiérge, “Cas extraordinaire d‘ichthyose genéralisée avec altérations des mu-
queuses buccale et nasale des cornées,” Annales, 1892, p. 717.
2 Jadassohn, “Ueber Pityriasis alba atrophicans,” Verhandl. der IV. Deutsch. Der-
matolog. Gesellsch., 1894, p. 392.
3 Hallopeau and Jeanselme, “Sur une ichthyose avec hypotrophie simulant une
sclérodermie,” Annales, 1895, p. 1016 (case demonstration).
4 Audry, “Sur les formes atrophicantes de l‘ichthyose et leur histologie," Jour. mal.
cutan., 1895, p. 265.
5 See also Joseph‘s paper, “Ueber ungewöhnliche Ichthyosisformen,” Verhandl.
der IV. Deutsch. Dermatolog. Gesellsch., 1894, p. 407 (case illustration and histologic
cut—case suggestive of both acanthosis nigricans and Darier‘s disease).
6 Macleod, “Three Cases of Ichthyosis Follicularis Associated with Baldness,” Brit.
Jour. Derm., 1909, p. 165, goes over this entire subject, reviewing various cases reported
(with references), and making a good attempt to clear up the nomenclature of the follic-
ular diseases in which horny spines or plugs occur.
ICHTHYOSIS
567
is generally noticed only toward the end of the first or second year,
it is quite probable, as already stated, that it is in reality always con
genital. I am inclined to share Hutchinson‘s1 belief on this point, “that
it usually takes its origin during intra-uterine existence, but that it may
be, in many cases, so slight at the time of birth that its presence is en
tirely overlooked. On the other hand, it may have already developed
to such a degree of severity that the infant is quite incapable of taking
on the functions of life for itself.” These latter represent those of the
so-called ichthyosis congenita already described. Exceptionally exam
ples of an ichthyotic condition of the skin have been noted in which the
development presented later in life, but these are usually open to ques
tion, although Crocker2 refers to a suggestive case of acquired ichthyosis
in a man aged seventy-four, in whom the sweat function became less
active or more or less in abeyance ten years previously, and the skin then
began to get dry and scaly, finally presenting appearances clinically
similar to those in the ordinary cases. In some instances the hereditary
predisposition is exhibited only in one or two of the children, but ex
amples of its occurrence in three and more members of the same family
have been recorded from time to time by various observers (Kaposi,
Crocker, Jeanselme, Frick, and others).3 Occasionally a predominant
family tendency to its appearance in those of one sex has been noted.
Both sexes are, however, its subjects in probably about equal proportion,
although most of the cases under my own observation have been males.
It is observed in all stations of society. It is not, however, a common
disease, although in its slight grade (xeroderma) it is doubtless more
frequent than it apparently seems. It is met with in all countries. In
districts where family intermarriage is not uncommon its relatively
more frequent occurrence is suggestive of an endemic character, as in the
Indian Archipelago, especially the Molucca Islands, referred to by
Hirsch,4 and also, according to Jablonowski,5 among two Albanian
tribes on the Adriatic shores. As Hirsch states, however, and as Jab-
lonowski‘s description indicates, it is probable that all these cases thus
referred to are not examples of this disease. In fact Henggeler6 has
rioted, in India, that most cases thought to be ichthyosis were cases of
tinea imbricata. A condition of the skin somewhat similar to that of
ichthyosis has been noted by Schuchardt7 in workers in paraffin. From
the absence of the thyroid in his case of “ichthyosis congenita,” Winfield
suggests further observation on this point as to possible etiologic rela
tionship.
Pathology.—It is the common opinion that ichthyosis is to be
1 Hutchinson, Archives of Surgery, 1891-92, vol. iii, p. 64.
2 Crocker, Brit. Jour. Derm., 1895, p. 217 (case demonstration).
3 Kaposi, Diseases of the Skin (English translation by Johnston), p. 440 (in a family
of 8 children, 5 affected); Crocker, Diseases of the Skin, third edit., p. 569 (5 in a
family of 10 children); Jeanselme, Annales, 1894, p. 1277 (4 out of 5 children); Frick,
Jour. Cutan. Dis., 1897, p. 19 (3 in a family of 4 children).
4 Hirsch, Handbook Geog. and Histor. Pathology, Syd. Soc Translation, 1886,
vol. iii, p. 666.
5 Jablonowski, abs.-ref. in Monatshefte, 1884, vol. iii, p. 383.
6Henggeler, “Ueber einige Tropenkrankheiten: Tinea Imbricata,” Monatshefte,
1900, vol. xliii, p. 325 (with excellent case illustrations).
7 Schuchardt, Volkmann's klin. Vorträge, No. 257 (Chirurgie No. 80), p. 2214.
568
HYPERTROPHIES
viewed as an inherited deformity of the skin rather than a disease.
The pathologic changes were originally considered seated essentially in
the epidermis, but later observations, however, tend to hold the surface
alterations as due, partly at least, to underlying processes in the corium,
especially of the connective tissue. That the nervous system is a factor
seems probable from the observations concerning examples of local dry-
ness and scaliness resulting from nerve injuries.. Leloir,1 who among
others considers the disease of trophoneurotic origin, found in 2 cases a
degenerative peripheral neuritis, and in 1 of these cases also degenerative
changes in the spinal roots. These observations have not, however,
been corroborated by others. The histologic characters have been
studied by various observers, the latest among whom are Esoff,2 Unna,3
Audry,4 Tommasoli,5 Giovannini,6 and others. Esoff found the increased
formation of epithelial scales, with heightened tendency to cornifica-
tion, and the greater thickness of the epidermis due principally to its
longer retention, the process of exfoliation being slowed. Degenerative
changes were also observed in both the coil and sebaceous glands.
Unna states that there is deformity of a weakly developed prickle layer
and of the papillary body, together with a much thickened horny layer.
The granular layer is everywhere absent on the surface of the prickle
layer, and there is absence of keratohyalin, the horny layer being formed
directly from the rete, without, as usual, the intervention of this sub
stance. The horny cells thus formed have no nuclei and are homo
geneous, there occurring, in fact, a special form of abnormal cornification.
In the changes in the tissue of the cutis the papillary body is sometimes
more cellular than normal, the cells often larger, as likewise the endo-
thelia and perithelia of the superficial capillaries, and also increased in
number. The collagenous tissue is thickened, and the lymph-spaces
correspondingly narrowed. A small collection of ordinary spindle cells
sometimes surrounds the hair-follicles. In the more severe cases the
cellular infiltration is more pronounced. The papillae are usually more
or less compressed and thus lengthened, sometimes being flattened.
He believes that the findings indicate a low inflammatory basis, is to be
ascribed to ichthyosis, and that it is not simply a thickening of the horny
layer. Tommasoli also found somewhat similar changes in the cutis,
as well as the usual changes in the epidermis. Audry did not, on the
contrary, find evidences of an inflammatory process; the granular layer
was considerably hypertrophied; the sweat-glands seemed unchanged,
but there was atrophy of the sebaceous glands. In a case investigated
by Giovannini the predominant changes were observed about the
periphery of the sweat-gland ducts, with mitosis of the epithelial cells
of the ducts.
1Leloir, Arch, de Physiolog., 1881, p. 405.
2 Esoff, “Beitrag zur Lehre von der Ichthyosis, etc.,” Virchow's Archiv, 1877, p.
417 (with histologic cuts and references).
3 Unna, Histopathology, p. 322 (with histologic cuts).
4 Audry, “Critique anatomique de quelques keratonoses,” Annales, 1893, p. 384.
5 Tommasoli, “Sur l‘histopathologie et la pathogenèse de l‘ichthyose,” Annales,
1893, P. 537 (with literature references).
6 Giovannini, Giorn. della R. Accad. de Med. di Torino, Dec, 1893, p, 653—abstract
in Annales, 1894, p. 1176.
ICHTHYOSIS
569
The process consists, in the simplex variety, of an accumulation
and thickening of the epidermis, but especially of the horny layer, and
often a somewhat thinned condition of the rete. The formerly con
sidered papillary hypertrophy is apparent, more than real, the irreg
ularities resulting from a dipping-down of the horny strata, the papillae
being thus compressed and elongated. In fact, the papillae themselves
often show atrophy. Slight evidences of inflammatory action are some
times found in the cutis, and the glandular structures in marked cases,
usually after long continuance of the malady, undergo degenerative
changes. There is, as a rule, poor. development of the panniculus adiposa.
The associated keratosis pilaris, often most marked in some of the milder
types, presents but little, if any, essential variation from that form which
occurs independently.
In ichthyosis hystrix, according to Schourp,1 the direct transition
from rete cells into horny cells without material intermediate change
is also noted. Kaposi (loc. cit.) states that the anatomic conditions in
this form of the disease do not differ from those in old warts: enor
mously elongated papillae, above which the horny layer is piled up in
thick, stratified coats. There is moderate cell-infiltration of the papillae,
with dilated vessels.
Diagnosis.—The features of ichthyosis are usually so character
istic that no difficulty arises in the diagnosis. The harsh, dry skin,
with thickened epidermis, and furfuraceous to plate-like scaliness, with
frequently follicular elevations (keratosis pilaris) or warty-looking
growths, its greater development upon the extensor surfaces, and the
absence of inflammatory symptoms, constitute a picture quite readily
recognized. Moreover, there is the history of the affection dating back
to infancy or earliest childhood, and its amelioration, or in mild type
complete, or almost complete, disappearance during the summer weather,
as corroborative evidence. It is to be borne in mind, however, that in
some instances, especially in cold, snappy, windy weather, eczematous
complications, more particularly, however, of exposed parts, is occasion
ally observed, and this fact should not be permitted to mislead. The
local character of the ichthyotic-looking skin in elephantiasis, as well as
the other associated symptoms, will prevent this latter being confused
with true ichthyosis. The same may be said as to the exceptional in
stances of eczema verrucosum of the region of the lower leg and ankle.
The features of ichthyosis hystrix are usually still more pronounced
and characteristic, and an error is scarcely possible. It should not be
confused with linear nævus.
Prognosis.—There is generally a slight, but often not mate
rial, increase in the condition up to the age of youth or early adult life,
after which it remains practically stationary, with sometimes trifling
improvement. The type once established, it practically remains un
changed, the mild, moderate, and severe varieties each continuing as
such. The outlook for the patient as regards a cure is unfavorable, as
may be inferred from what has already been said, but the process in
ichthyosis simplex may usually be kept more or less in abeyance, or
1 Schourp, “Ueber Ichthyosis hystrix,” Dermatolog. Centralblatt, 1898, p. 242.
570 HYPERTROPHIES
rendered endurable by proper measures. The disease continues through
out life, and, so far as I know, but two exceptions to this are on record—
by Hebra1: in one instance of an ichthyosis simplex in a girl of eight,
which disappeared permanently in consequence of an attack of measles;
the other, the hystrix variety, after an attack of variola. It is not im
possible that if treatment were begun in early life and perseveringly con
tinued, in the milder varieties at least, a favorable result might be
brought about.
Treatment.—The treatment of ichthyosis is essentially external,
but first a few remedies occasionally administered internally should
be referred to. Of the several so employed, those which seem at times
to have a favorable, though temporary, influence are pilocarpin and
thyroid extract. In several instances it has seemed to me that pilo-
carpin or jaborandi, administered in dosage sufficient to stimulate the
sweat secretion, has tended to make the skin more supple and the
scaliness less marked. Thyroid is a preparation that deserves trial,
in view of the favorable, though admittedly temporary, influence re
ported by Don,2 Bramwell,3 Abraham,4 and a few others. Hardaway5
believes that he has seen some effect in mild cases from the adminis
tration of two or three Garrod‘s sulphur tablets daily. Fagge6 recom
mended antimonial wine. In those of impaired nutrition cod-liver oil
seems to be of some slight service. Sherwell7 thought the administration
of linseed to be of advantage. After all, the treatment which must
always be adopted in these cases, if certainty of amelioration or relief
is desired, consists in external measures, and these, if properly followed
up and continued, will often bring about the appearance of an apparently
normal skin. When this is effected, treatment is to be continued, but
much less rigorously. There are especially two objects to be kept in
mind in the management of these cases—removal of the scaliness and
the maintenance of a soft and pliable condition of the skin. For the first,
frequent baths will often suffice. These baths will, according to the
severity of the case, be either plain warm baths, alkaline baths, or hot-
water baths with the free use of sapo viridis—the same, in fact, as used
in psoriasis. Steam and hot-air baths may also be had recourse to for
rapidity of action or in cases in which there is considerable firm epidermic
thickening. After each bath the skin should be rubbed or anointed with
a mild salve or oil. In the mildest cases the baths alone will serve to
keep the skin in an apparently normal state; in the others, and always
in the more severe cases, an oily application should be made after each
bath. A weak glycerin lotion, from \ dram to 2 drams (2.-8.) to the
ounce (32.) of water, oil of sweet almonds, cold cream, benzoated lard,
petrolatum, or the like will answer for this purpose. The addition of
1 Hebra and Kaposi, Hautkrankheiten, 1876, vol. ii, p. 41.
2 Don, Brit. Med. Jour., 1897, ii, p. 1334.
3 Bramwell, Brit. Jour. Derm., 1894, p. 205.
4 Abraham, ibid., 1896, p. 106 (discussion).
5 Hardaway, Manual of Skin Diseases, second ed., p. 261.
6 Fagge, quoted by Pye-Smith, Diseases of the Skin, p. 284.
7 Sherwell, “The Use of Linseed and Linseed Oil as Therapeutic Agents in Diseases
of the Skin,” Arch. Derm., 1878, p. 303.
POROKERATOSIS
571
lanolin in the proportion of from 15 to 30 per cent, to one of the oint
ments named will sometimes prove an advantage. In most cases the
incorporation of from 10 to 40 grains (0.65-2.6) of salicylic acid to the
ounce (32.) of ointment will be found more effective. A satisfactory
ointment is one consisting of 10 to 40 grains (0.65-2.6) of salicylic acid,
glycerin 20 minims (1.35), lanolin 2 drams (8.), benzoated lard and pe
trolatum, each, 3 drams (12.). The quantity of salicylic acid depends
upon the amount and rapidity of scale accumulation. The addition
of resorcin, 3 to 10 per cent., is an advantage; this drug, applied in oint
ment of 3 per cent, strength in mild cases, and 5 to 20 per cent, in
markedly developed cases, has been strongly recommended by Andeer1
and indorsed by Jamieson.2 The latter considers it superior to the sul
phur ointment plan. Unna3 speaks well of a course of treatment con
sisting of the daily application of sulphur ointment of variable strength,
usually 5 to 10 per cent., and also of ichthyol applications, 10 per cent.,
with water or in ointment, and frequent baths; he refers to several cases
in which the good results remained for several months or longer after
active measures had been discontinued. Occasional sulphur vapor
baths in conjunction with the milder ointment and bath plan will
sometimes prove of additional benefit.
In ichthyosis hystrix, alkaline, steam, hot-air, and sulphur baths,
together with the use of the strong salicylic acid ointment, will, in the
milder varieties, usually suffice to clear off the horny accumulation.
Sometimes, however, the formation is so hard and adherent that the
application of salicylic acid plasters, 10 to 25 per cent, strength, is re
quired, and in extreme cases it may be necessary to have recourse to
caustics or to the knife.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |