| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
ANGIOKERATOMA l
Synonyms.—Keratoangioma; Lymphangiectasis (Colcott Fox); Fr., Verrues
télangiectasiques (Dubreuilh); Tuberculides angiomateuses (Leredde); Ger., Angio-
keratom.
Definition.—An affection usually of the extremities, occurring,
for the most part, in those subject to chilblains, and characterized by
the appearance of telangiectases which subsequently develop into warty-
looking elevations.
Symptoms.—The descriptions of Cottle, Mibelli, Pringle, Zeisler,
Fordyce, and others have given a pretty clear picture of the symp
tomatology of this rare malady. It generally follows one or more
attacks of chilblains, minute vascular dilatations or telangiectases sub
sequently arising. They are pinpoint to pin-head in size, discrete, or
in close proximity or crowded together. At first they may be pinkish
in tinge, later becoming darker and even with a dark-purplish hue or
color, the central point usually being the darkest; occasionally the color
partakes of a reddish brown. The backs of the fingers and the dorsal
surface of the toes, and especially toward the basal portions, are the
favorite sites; the lesions may occasionally appear on the palmar sur
faces also. Exceptionally they are seen elsewhere, as in Fordyce's and
Sutton‘s cases, in which the lesions were confined to the scrotum, and
in Anderson's patient, of more or less general distribution. In Zeis-
ler's case, in addition to the ordinary lesions on the hands and feet,
the auricles, forearms, and legs were the seat of pedunculated vascular
tumors and. nævus-like patches. The fingers and hands have been,
however, the most frequent localization.
1 Literature: Cottle, St. George‘s Hosp. Reps., 1877-78, vol. ix, p. 758, with colored
illustration; Pringle, Brit. Jour. Derm., 1891, pp. 237, 282, and 309 (with 2 colored
plates and histologic cut, and a résumé of previously reported cases); Zeisler, Trans.
Amer. Derm. Assoc. for 1893 (abstract; full paper not published); Fordyce, Jour. Cutan.
Dis., 1896, p. 83 (with a colored plate and 5 excellent photomicrographs, and complete
literature references to above reports and those of Mibelli (1889), Crocker (1888 and
1891), Colcott Fox (1886 and 1889), Dubreuilh (1889 and 1893), Audry (1893),
Deydier (1892), Brocq (1892), Thibiérge (1892), Joseph (1892 and 1894), Tommasoli
(1893), Renault (1894); Dubreuilh, Annales, 1896, p. 1202; Mibelli, Monatshefte, 1897,
vol. xxiv, p. 428; Wisniewski, Archiv, 1898, vol. xlv., p. 357 (with 2 colored histologic
cuts, review of the subject, and references); W. Anderson, Brit. Jour. Derm., 1898, p.
113 (general distribution, with almost complete immunity of the hands and feet; 2 cuts
showing distribution, and 1 of histology); Dore, ibid., 1903, p. 23 (with chilblain circu
lation, erythema pernio, and erythema induration); R. L. Sutton, Jour. Amer. Med.
Assoc, July 15, 1911, p. 189 (a clinical and histopathologic study of angiokeratoma
of the scrotum with case illustration, review, and references).
576
HYPERTROPHIES
After a while the telangiectases show slight elevation, and the
surface may become rough and irregular and somewhat horny, and
present, more especially when close or bunched together, a warty
aspect, the resemblance to small warty growths leading Dubreuilh to
designate the malady “telangiectatic warts.” Closely lying vascular
dilatations sometimes practically fuse together, forming a slightly raised
patch, a fractional part of an inch in diameter, with small projecting
or irregular horny elevations, the reddish or purplish color being most
marked peripherally. Different stages of the process are usually to be
seen, from the passive, livid congestion of chilblains to the well-marked
warty character. As a rule, the color may partly, rarely completely, be
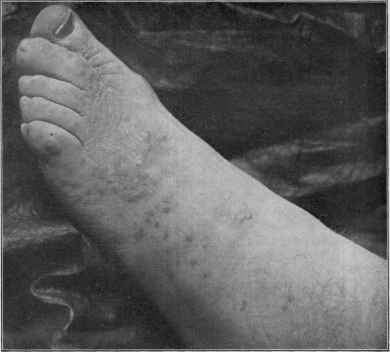
Fig. 138.—Angiokeratoma.
made to disappear on pressure. The condition is commonly worse
during the cold season, at which time new points are more apt to appear.
Thus the malady tends to become more widespread, the growths show
ing no signs of retrogression. There are no subjective symptoms, and
beyond the disfigurement, the malady gives rise to no trouble, although
the larger projecting growths, if roughly knocked, may show a disposition
to bleed.
Etiology and Pathology.—The disease is rare, although some
what similar scattered single lesions, lacking distinct horny characters,
are occasionally seen on the hands and upper trunk. The malady
usually begins in childhood or youth, although in Fordyce‘s patient,
ANGIOKERATOMA
577
aged sixty, it had apparently begun much later, and Zeisler's case—a
male—began when aged forty-nine. The female sex seems to furnish
the majority of cases. In some instances more than one member of
the family has exhibited the disease; according to Dubreuilh,1 Mibelli
saw 6 cases in the same family, and Pringle2 saw 4—all males. Local
circulatory weakness, as that resulting from chilblains, is apparently an
important factor in most instances, although in the 2 cases reported by
Fordyce and Anderson this preliminary feature was wanting; in Fordyce‘s
case, however, the patient had a double varicocele, indicating a tendency
to blood-vessel dilatation. In some instances, however, there was no
apparent cause.
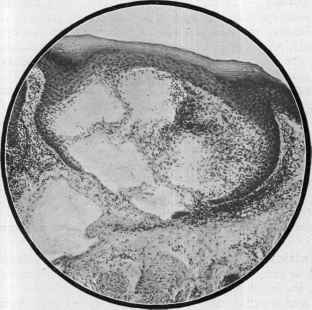
Fig. 139.—Angiokeratoma (X about 100), showing cavernous space filled with
blood-corpuscles and divided by fibrous septa; hypertrophy of the corneous layer and
rete (courtesy of Dr. J. A. Fordyce).
Mibelli, who gave the present accepted name to the malady, was
the first to investigate the pathologic histology, since which time his
findings have for the most part been corroborated by Pringle, Joseph,
Audry, Wisniewski, Fordyce, Unna, and others. The primary patho
logic change is a vascular one, the keratosis, a secondary phenomenon.
The lesions, quoting Fordyce‘s words, consist of lacunar spaces filled
with blood, occupying the papillary portion of the derma, some of which
are found inclosed in the rete; and these cavernous spaces are evidently
the essential, and probably primary, feature of the disease. It is
probable, as Mibelli and Pringle suggest, and in which opinion Fordyce
1 Dubreuilh, loc. cit.
2 Pringle, Brit. Jour. Derm., 1913, p. 40 (case demonstration); 4 cases, father and
three sons, quite typical on the hands, and to a less degree on the feet also.
37
578
HYPERTROPHIES
is inclined to coincide, that the lacunar dilatations result from changes
in the papillary vessels, superinduced by causes which impair the con
tractility of the vessel-walls, the most common being attacks of chil
blains. Fordyce's investigations lead him to coincide in Pringle's
hypothesis that the blood-spaces in the rete Malpighii are caused by a
downgrowth of the cells of this layer, producing a constriction of the
terminal loops and their resulting distention. In addition to these several
changes, there is a slight inflammatory infiltration to the underlying
derma and thickening of the corneous layer. Differing from other
observers, Mibelli and Audry found also some dilatation of the lymph-
spaces.
Diagnosis.—The primary minute telangiectases and subsequent
warty tendency, with the associated dark-red or purplish color and
the localization, together with often a history of previous exposure to
severe cold, with consequent chilblains, are usually sufficiently diag
nostic. The vascular dilatation is entirely wanting in ordinary warts,
and the growth and appearance of the latter different.
Prognosis and Treatment.—The malady is persistent, with
no tendency to involution. The treatment consists, as successfully em
ployed by Pringle, of electrolysis, each lesion receiving attention, the
needle being attached to the negative pole, and a current of 2 or 3 mil-
liampères used. Measures should be advised as to proper hand and
foot covering in cold weather, and the maintenance of circulatory tone
by exercise and suitable tonics if indicated.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |