| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
VARIOLA
(W. M. Welch)
Synonyms.—Smallpox; Fr., Petite-vérole; Ger., Blättern or Pocken; Ital., Vajuolo.
Definition.—Smallpox is an acute infectious disease character
ized by an initial fever of about three days’ duration, succeeded by an
eruption passing through the stages of papule, vesicle, and pustule,
ending in incrustation, and leaving pits or scars; the fever either inter
mitting or remitting in the papular, and increasing in the pustular,
stage.
Symptoms.—The period of incubation of smallpox is seldom less
than eight days or more than fourteen, commonly from ten to twelve
days. The symptoms constituting the initial stage, or stage of invasion,
are usually ushered in suddenly and often with considerable violence.
Among the earlier symptoms is a distinct chill, which may be mild or
severe, and which is immediately followed by rise of temperature. The
thermometer often registers 1030 or 1040 F. on the first day, and may
be a little higher on the succeeding days. The pulse and respirations
keep apace with the febrile movement. Prostration is often extreme.
Vertigo on assuming the erect position is a frequent symptom. At this
time vomiting and epigastric tenderness are commonly observed. Head
ache usually begins at the onset of the disease, and continues until the
appearance of the eruption. It may be excruciating, and, when the fever
is high, accompanied by delirium. Convulsions are very common in
children, and at times there may be coma. Pain in the lumbar and
sacral regions comes on early, and, like the headache, subsides at the
beginning of the eruptive stage. This symptom is not invariably present,
although it occurs in over one-half of the patients. In hemorrhagic cases
the backache is often violent. A peculiar prodromal rash, varying in
frequency in different epidemics, often makes its appearance on the
second day, and disappears within forty-eight ‘hours. It is stated by
some authors to be scarlatiniform in character, but in my experience it
has more often resembled measles, and has been designated “roseola
variolosa.” I have observed this rash more frequently in varioloid
than in severe cases of variola.
The eruption usually appears upon the third day of illness, mani
festing itself first upon the face, particularly about the forehead, temple,
and mouth, and then rapidly appearing upon the scalp, neck, ears,
forearms, and hands. In the course of twenty-four hours the body and
VARIOLA
48l
lower extremities become involved. The eruption continues to increase
for two or three days before its definite limit is reached. The lesions
consist at first of minute red points, which in the course of twenty-four
hours develop into elevated papules with characteristic shot-like indura
tion. On the third day of the eruption many of the lesions will be found
to contain a little clear serum, and by the fourth or the fifth day all the
papules will have been converted into vesicles with cloudy or milky
contents. These continue to enlarge, attaining their maximum size
about the seventh or the eighth day. Many of the vesicles will be seen
to have the central depression or umbilication, which is a feature of
diagnostic value.

Fig. 118.—Well-marked discrete smallpox on ninth day, showing lesions in the stage
of beginning crust-formation (courtesy of Dr. J. F. Schamberg).
The stage of suppuration usually commences about the sixth day,
when the contents of the vesicles are yellowish and decidedly puriform.
In the process of development the pustules lose their umbilication and
become large and globular. The reddish areola, which at first surrounded
the lesions, acquires greater breadth and a more intense hue. Where
the pustules are thickly set, as upon the face, great swelling and intumes
cence take place, so distorting the patient‘s features as to render him
completely unrecognizable. The eyelids are frequently so edematous
as to preclude the possibility of their being opened. The lips, nose, and
ears are greatly tumefied, and the scalp is swollen and painful. The
mucous membranes are also attacked, the lesions manifesting themselves
upon the lips, buccal and nasal mucous membrane, tongue, pharynx,
and at times the larynx.
31
482
INFLAMMATIONS
• Upon the appearance of the eruption, or, more commonly, on the
second or the third day thereafter, the temperature falls, the head
ache, backache, vertigo, vomiting, etc., cease, and the patient believes
himself on the road to convalescence. The subsidence of these symptoms,
however, except in mild cases, is only temporary, for upon the commence
ment of the stage of suppuration the temperature again begins to rise
and continues high until the decline of the suppurative fever. The
height of the fever is proportionate to the extent of the eruption, the
temperature varying from 1020 F. in mild cases to 1040 or 1050 F. in
confluent smallpox. Headache, restlessness, and delirium are common
during this stage, the patient at times sinking into the typhoid state.
During the stage of desiccation, which begins about the eleventh
or twelfth day, the tumefaction subsides, and the normal contour of
the features is gradually restored. The contents of the pustules dry
into crusts, which process is often accompanied by intense itching.
The crust-formation begins in the center of the pustules, leading to a
secondary umbilication. In regular cases of variola vera the shedding
of the scabs requires a period of three to four weeks, making the entire
duration of the disease about five or six weeks. After the scabs have
fallen the skin presents a red, spotted appearance, and is disfigured by
scars or pits. These are deepest on the face, particularly about the end
and alæ of the nose. The hair is often lost, but thorough restoration
usually follows.
The clinical history of smallpox is not complete without reference
to other forms and varieties of the disease. The above description
; relates more particularly to cases in which the eruption is either dis
crete or semiconfluent. The grades of smallpox cover a wide field of
variation, from an eruption consisting of but a few small pustules,
scarcely sufficient to identify the disease, to an eruption completely
covering the entire cutaneous surface. During the past few years there
has appeared in this country an epidemic of smallpox so unprecedentedly
and uniformly mild as to constitute an unwritten chapter in the history
of the disease. Its benignancy can be best estimated when it is stated
that the mortality-rate among many thousand vaccinated and unvac-
cinated cases throughout the United States during the first three months
of 1901 was not much over 1 per cent. The clinical picture is that of
mild varioloid, despite the absence of any such modifying influence as
commonly exists in this form of the disease. Therefore a brief descrip
tion of varioloid will suffice to portray also this unusually mild form of
smallpox.
The prodromal symptoms of varioloid may be severe or mild; in
the latter case it being possible to prophesy a sparse eruption. The
duration of the initial stage is more variable than in variola vera, varying
from twenty-four hours to five days. The eruption of varioloid differs
from that of variola only in that it is milder in its course and shorter in
duration. The lesions may be limited to a very few on the face, or they
may be semiconfluent. In the milder forms the lesions may become
abortive at an early period; in the severe forms the evolution of the lesions
may not differ from unmodified smallpox. The cutaneous involvement
Plate XVI.
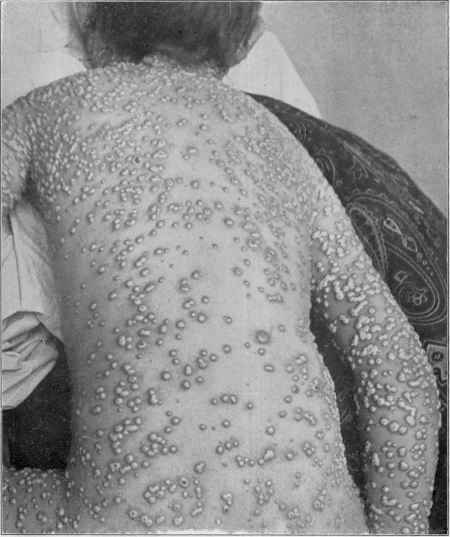
Variola—an extensive case showing numerous lesions on trunk as well as face and
extremities (courtesy of Dr. G. W. Wende).
VARIOLA 483
is often superficial, being limited to the upper layers of the skin. As
a result, we have a shorter eruptive course, earlier desiccation, more
rapid shedding of the scabs, and fewer and less disfiguring scars. Occa
sionally the lesions develop into large, solid papules, conic in form, with
vesicular summits. On shedding of the crusts, instead of pits, tuber-
culated or warty-looking excrescences are left. These, however, flatten
down and disappear in the course of time. Secondary fever is either
absent or trivial in character.
The eruption of confluent variola is usually preceded by severe
prodromes, such as high fever, intense headache and backache, vomit
ing, etc. The temperature does not descend as low on the appearance
of the eruption as in milder cases, nor does the remission continue so
long. On account of the extensive involvement of the skin, redness and
swelling begin early, the former as early as the second day. Many of

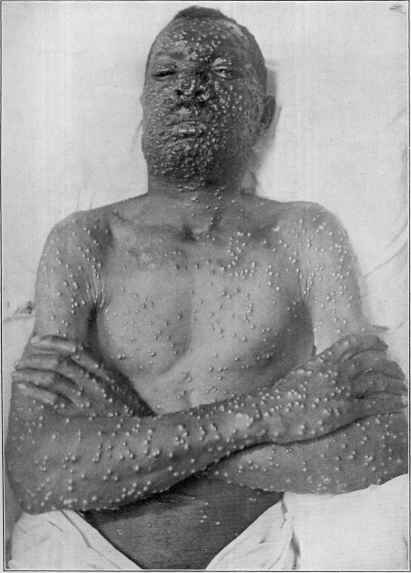
Fig. 119.—Variola—moderate case (courtesy of Dr. G. W. Wende).
the thickly set papules coalesce, and in the formation of vesicles the
confluence is so great as often to cover almost the whole cutaneous sur
face. The confluent pustules are usually flat, and sometimes present a
milky or pasty appearance. At the height of the eruption the patient
is unrecognizably disfigured. The mucous membranes of the nose,
mouth, pharynx, and larynx are often intensely involved. The soft
palate, tonsils, and tongue may become greatly swollen, and edema of
the glottis may lead to a fatal termination. Upon rupture of the pustules
and decomposition of the contents the stench often becomes unbearable.
Secondary fever is usually very high, and death frequently occurs at this
period from septicemia and exhaustion. When recovery takes place,
convalescence is long and tedious, and apt to be interrupted by the occur
rence of boils and abscesses.
The names petechial, purpuric, and hemorrhagic variola are applied
to the different phases presented by malignant smallpox. A pete-
484
INFLAMMATIONS
chial rash is sometimes seen at the close of the initial stage, about the
time the true eruption appears or should appear. This is quickly
followed by the purpuric or hemorrhagic lesions, which lead rapidly
to a fatal termination. At other times petechiæ and ecchymoses appear
between the papules or vesicles, the latter often filling up with a san-
guinopurulent fluid. Variola purpurica is the most malignant form of
the hemorrhagic type. At the end of the initial stage, which is par
ticularly characterized by intense backache and excessive prostration,
a diffuse scarlatinoid efflorescence appears on various parts of the trunk
and extremities. This gradually assumes a dark-red or purplish colora
tion, which does not disappear on pressure. In addition, petechiæ,
vibices, and ecchymoses occur. The face soon becomes involved,
presenting a swollen and puffy appearance. Indistinct sanguinolent.
vesicles, blackish or leaden-gray in color, may be seen in various localities.
As the disease progresses, the skin becomes almost black or a deep indigo
color. Hemorrhages occur from the various mucous membranes.
Death is the almost inevitable termination. In the form designated
variola hæmorrhagica pustulosa the vesicles, instead of filling with
purulent material, contain a bloody fluid. This condition of the vesicles
may be limited to certain localities or may be generalized, with petechiæ
and ecchymoses interspersed. Hemorrhages occur from the nose,
mouth, and intestinal and urinary tracts. This form runs a somewhat
longer course than purpura variolosa, but is almost as certain to end
fatally.
Among the common complications and sequelæ of smallpox may
be mentioned erysipelas, boils, abscesses, and disease of the eyeball,
middle ear, respiratory tract, and joints. Erysipelas occasionally
comes on during desiccation, and is apt particularly to involve the face.
Pneumonia sometimes occurs. Furuncles and abscesses are extremely
common. But few patients pass through a well-marked attack of small
pox without suffering from boils during the later stage of the disease.
Gangrene of the skin, especially of the scrotum, is a complication which
usually leads to a fatal termination.
Diagnosis.—In the initial period of the disease great assistance
may be gained by determining the presence or absence of vaccine marks
and their number and character. Furthermore, by ascertaining whether
or not smallpox is prevalent, and whether the patient has been exposed
to the disease. During the eruptive stage variola may be confounded
with varicella, pustular syphiloderm, impetigo contagiosa, drug-rashes,
etc.
The onset of varicella is very different from that of variola. There
is usually no distinct febrile stage preceding the eruption. It is true
that in many cases of extremely modified smallpox no reliable history
of an initial stage can be obtained, so that in such cases the diagnosis
must be made from the appearance and behavior of the exanthem alone.
It is important to bear in mind the following facts: that the lesions of
varicella make their appearance as distinct vesicles containing perfectly
clear serum; that they are usually seen first on parts of the body covered
with clothing, and especially on the back, where they are apt to be most
Plate XVII.
Variola on the seventh day, showing the usual preponderance of lesions on the face,
hands, and wrists (courtesy of Dr. J. F. Schamberg).
VARIOLA
485
abundant; that they make their appearance in successive crops, and
may be seen in every stage of development; that they vary very greatly
in size; that they are unilocular and have an epidermal covering so deli
cate as to be readily broken by the finger-nail; that they are rather soft
and velvety to the touch; that many of them enlarge to a considerable
circumference by peripheral expansion, while others are as small as millet
seeds; that they are not umbilicated except by desiccation beginning
in their centers; that they run their course to the formation of crusts
in two to four days; that the crusts are thin, brown, and friable, and
when they have fallen off, red instead of pigmented spots remain; and
that but few of the lesoins are followed by permanent scars. The exan-
them of smallpox, on the other hand begins in the form of papules which
are firm and dense to the touch, feeling somewhat like grains of sand
buried in the skin; that they usually appear first on the face and then
on other parts of the body; that the papules slowly develop into vesicles
with milky or turbid contents; that the vesicles in well-marked cases
are umbilicated; that they are multilocular and have an epidermal cov
ering so dense as not to be easily broken by the finger-nail; that the
eruption prefers the exposed parts of the body, such as the face, hands,
and arms, being often only sparsely seen on the trunk; that the vesicles
are usually quite uniform in size; that they change into pustules; that
the eruption requires in severe cases twelve or more days to pass through
its various stages, while in extremely mild cases not more than five or
six days are required; that the crusts which form are thick and very
dark, and when they have fallen off, there remain pigmented spots and
more or less pitting.
Despite the above differentiation, it must be admitted that small
pox may occur in a form so atypical as to make the differential diag
nosis a matter of great difficulty. In such cases the patient should be
isolated and carefully watched for a few days, when the nature of the
disease will, as a rule, be easily determined.
The lesions of the pustular syphiloderm frequently resemble very
closely those of smallpox. The difficulty of diagnosis is often increased
from the fact that the eruption in syphilis is not infrequently preceded
by fever and various aches and pains, and that the lesions begin as
papules and end in pustules. Instead of appearing all at once, the
eruption of syphilis usually comes out in successive crops. Pustular
syphiloderm, however, may be distinguished by the milder constitu
tional symptoms during the initial stage; by appearance of the lesions
in successive crops; by the formation, at the summits of the papules,
of small vesicles which later become pustular; by the large indurated
base of each vesicle; by the absence of typical umbilication; by the
tendency to ulceration of some of the lesions; by the slower course of the
eruption, and by concomitant symptoms of syphilis and a history of
infection. In doubtful cases a few days’ observation of the patient will
usually suffice to determine the question; and the examination for
the spirochæta pallida and the Wassermann test can now also be
resorted to.
Impetigo contagiosa has been confounded at times with the mild
486 INFLAMMATIONS
variola of recent years. It may be easily differentiated by the absence
of fever, by the usual limitation of the lesions to the face and hands,
by the fact that they are primarily vesicular or bullous, rapidly becoming
pustular and drying into flat, ocher-colored crusts, and by the extreme
superficiality of the process.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |