| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
URTICARIA
Synonyms.—Hives; Nettlerash; Fr., Urticaire; Ger., Nesselsucht; Nesselaus-
schlag.
Definition.—Urticaria is an inflammatory affection characterized
by evanescent whitish, pinkish, or reddish elevations or wheals, some
what variable as to size and shape, and attended by itching, stinging,
and pricking sensations.
Symptoms.—The eruption in urticaria usually comes out sud
denly, occasionally being preceded by burning or itching of variable
intensity. It is erythematous in character and consists of scanty or
profuse pea- to bean-sized elevations, linear streaks, or small or large
irregular patches, or an admixture of these forms. It may be limited
in extent and distribution, or more or less general and abundant. While
no part of the body is exempt from possible manifestations, covered
parts, especially the lower trunk, buttocks, and upper outer chest, around
about the axillary regions, are favorite localities. The outbreak may
be preceded and accompanied by symptoms of gastric derangement, and
exceptionally and in extensive and markedly acute cases by some febrile
action. In many cases, however, the cutaneous eruption is unaccom
panied by any other recognizable symptoms. The lesions are fugacious
in character, disappearing and reappearing in the most capricious manner.
They are somewhat firm, with an average size in the typical wheal of a
flattened large pea. They may vary in tint in different cases, and in
different lesions in the same case. They are pinkish or reddish, with
usually a whitish central portion. At times they are almost entirely
whitish, with a narrow, pinkish areola. The subjective symptoms are,
as a rule, quite marked, consisting of stinging, intense burning or itching,
or a combination of these symptoms. Rubbing or scratching the parts
to obtain relief will ordinarily provoke a new outcropping in such regions.
The lesions are distinctly evanescent, lasting from several minutes to a
fractional part of a day, the average being about an hour or two. The
intervening skin is perfectly normal in appearance, new lesions present
ing rapidly from time to time. In exceptional cases the individual
lesions may persist for several days or a week or longer—urticaria per-
stans. In some instances, with or without a few or more wheals on other
parts, the disease presents itself as an ill-defined pufrmess of the hands
1 Marquez, Gaz. hebdom., 1889, p. 91.
180
INFLAMMATIONS
and fingers and feet, accompanied with intense subjective symptoms of
burning and itching.
During an outbreak of urticaria, and in exceptional instances with
out actual outbreak, and even in the interim of attacks, it is possible in
some persons to bring out linear wheals by simply rubbing the finger or
drawing a lead-pencil somewhat firmly over the surface. In this manner
letters, symbols, and words may be produced at will and last for minutes
or hours. This, or a phase of it, constitutes the so-called urticaria
factitia, dermatographism, autographism.
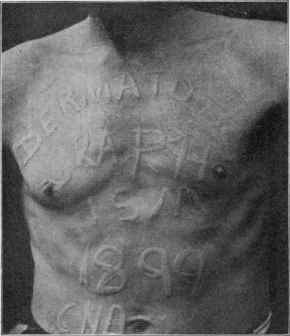
Fig. 34.—Dermatographism. Tracing done with the blunt end of a lead pencil,
making slight pressure, the “welts” reaching full and prominent development in
several minutes (courtesy of Dr. C. N. Davis).
Barthélemy1 has thoroughly studied this peculiar condition, and
finds that while it is commonly associated with urticarial attacks at
short or long intervals, it not infrequently may exist independently, and
the subject learn of its existence only accidentally. One such instance
as the last named has come under my notice. The lines or figures
brought out at will in these cases last a variable time—from twenty or
thirty minutes up to twenty-four hours. The tendency in some in
stances, according to Barthélemy, occasionally disappears temporarily.
The eruption in urticaria is not always confined to the external
surface. The mucous membranes of the mouth, throat, larynx, and
1 Barthélemy, Etude sur le Dermographisme ou Dermoneurose Toxivasomotrice,
Paris, 1893 (an admirable and complete monograph with a review bibliography of the
literature and notes of many cases and 17 illustrations).
URTICARIA 18l
possibly the intestinal mucous surfaces, may exceptionally be the seat
of wheals and edematous swellings, a number of instances of which have
been recorded, more especially in recent years (Delbrel, Madison Taylor,
Hinsdale, Merx, and others).1 Occurring about the throat and larynx,
the symptoms are sometimes alarming.
Urticaria may be acute or chronic; in most instances the former,
the outbreak coming on rapidly, with slight variations as to the intensity
of the attack. The lesions may continue to appear and disappear in the
most capricious manner, for several hours to two or three days, and then
disappear entirely; or there may be one more or less extensive outcropping
of wheals, reaching its acme in an hour or so, and then gradually fading
away. The duration of an acute attack is from several hours to several
days, the average being twenty-four to forty-eight hours. It may
recur in some instances from time to time at intervals of weeks or months
upon exposure to the necessary etiologic factor or factors. In exceptional
cases of urticaria, but more particularly in the hemorrhagic form, pig
mentation results which may last for some months or longer.
Chronic urticaria, fortunately, is not very common. In these cases
the lesions are usually evanescent, as in the acute type, and very often
somewhat scanty, but fresh efflorescences continue to appear from day to
day and from week to week almost indefinitely, the patient‘s general
health often suffering from the constant worry and discomfort produced
by the itching and burning.2 Very exceptionally the lesions, or some of
them, instead of being evanescent, are somewhat persistent, lasting days
or weeks—urticaria perstans (Pick); some cases of which are doubtless
examples of prurigo nodularis. Other instances of persistence of the
lesions, some assuming annular and gyrate forms, have been described
as urticaria perstans annulata et gyrata, but these cases seem to belong
more properly to erythema multiforme (q. v.).
Instead of the characteristic lesions of the disease, the eruption
may be atypical, thus arising the types known as giant urticaria, papular
urticaria (urticaria papulosa), hemorrhagic urticaria (urticaria hæmor-
rhagica, purpura urticans) bullous urticaria (urticaria bullosa).
The conditions variously described as giant urticaria, urticaria
tuberosa, urticaria œdematosa, and acute circumscribed edema are
closely allied or identical, varying usually as to degree, and presenting the
cutaneous symptoms of tumor-like swellings of evanescent character.
1 Delbrel, “Contribution a l‘etude de l‘urticaire des voies respiratoires,” These de
Bordeaux, 1896 (reviews 25 cases from literature and adds 2 of his own); Madison Tay
lor (larynx and skin), Philadelphia Med. Jour., April 2, 1898; Hinsdale, Philadelphia
Polyclinic, July 30, 1898; Freudenthal (recurrent and chronic of larynx and skin), New
York Med. Jour., Dec 31, 1898; Chittenden (buccal, pharyngeal, and nasal mucous
membrane and skin, chronic in character, with recurrent hematemesis), Brit. Jour.
Derm., 1898, p. 158; Goodale and Hughes (chronic and of tongue only, controlled by
salol), Amer. Jour. Med. Sci., April, 1899; Merx (recurrent, tongue, throat, and skin;
with bibliography), Munch, med. Wochenschr., 1899, p. 1174; F. A. Packard, Soc‘y
Trans., Philadelphia Med. Jour., July 22, 1899, and Archives of Pediatrics, 1899, P-
729 (showing apparent connection between respiratory disturbances and urticarial
eruptions).
2 Under the name “urtica solitaria” Vörner (Dermatolog. Zeitschr., Jan., 1913, p. 1)
records several (4) cases where general recurrent urticarial attacks finally gave place
to an occasional appearance of a single lesion, and usually when recurring this lesion
always appeared in the same place.
182
INFLAMMATIONS
They are frequently a part of a more or less general urticaria in which
most of the symptoms are of the ordinary wheal type, presenting the
edematous swellings here and there, more especially about the eye
lids, mouth, and ears. Occasionally, however, acute circumscribed
edema seems to be entirely or sufficiently independent of urticarial
manifestations, and free from subjective symptoms, to be entitled to
separate description (q. v.).
Urticaria papulosa, also known as lichen urticatus, consists essen
tially of an urticaria in which the lesions are discrete and scattered
and usually upon the limbs. They may appear as small, more or less
typical wheals, which disappear, leaving behind persistent eczema-like
papules, though somewhat larger than the papules in the latter disease.
Or the lesions may, for the most part, appear as papules from the start,
with here and there a scattered typical wheal. In addition to the serous
exudation of the ordinary wheal, there seems to be in this type a mark
edly inflammatory element. These papules usually itch intensely, and
as a result the summits of many of them are scratched and covered with
minute blood-crusts. They disappear but slowly, new papules coming
out from time to time. This type may last from one to several months
or longer, and tends to recur. It is almost entirely confined to young
children and to those in a depraved state of health. It is rather rare in
this country. 1 It is possible that this form, instead of being a true urti
caria, may be an example of mild prurigo, a disease which is not uncom
mon in Austria and other European countries.
Urticaria hæmorrhagica seu purpura urticans is characterized by
efflorescences similar in size and shape to those of ordinary urticaria
except that there is a variable amount of hemorrhage into the wheals.
It is probable that in the majority of these cases the purpuric condition
is the primary one, and the wheal formation secondary; in fact, in some
cases the purpuric element may be of a somewhat grave character, with
hemorrhages from the mucous membranes.
Urticaria bullosa, or bullous urticaria, is that form of urticaria in
which the lesions become capped with a vesicle or bleb or in which
the wheals are rapidly displaced by blebs. This anomaly is seen most
frequently upon the extremities, although this lesion may in excep
tional instances constitute the larger part of the eruption—so much
so as to suggest pemphigus, dermatitis herpetiformis, or bullous ery
thema multiforme. Apparently the inflammatory action has been
sufficiently great to give rise to considerable fluid effusion, in this manner
the wheals resulting in the formation of bullæ.
Etiology.—Urticaria may occur at all ages and in both sexes,
and in all countries. It is much more frequent, however, between
the ages of early childhood and middle adult age, and is possibly some
what more common in the female sex. The papular type is more fre
quent in England2 than elsewhere, and is almost exclusively seen in
1 Chipman, California State Jour, of Med., June, 1910, states that it is not uncom
mon in San Francisco, and thinks the flea is frequently a factor there in its pro
duction.
2 Colcott Fox, “On Urticaria in Infancy and Childhood,'’ Brit. Jour. Derm., 1890,
pp. 133 and 176.
URTICARIA
183
children. There are many causes, but there is some peculiar individual
predisposition necessary, inasmuch as the same cause may not produce
the eruption in different subjects. In some instances a hereditary in
fluence or predisposition is observed, especially in the cases associated with
giant lesions and edematous swellings. The etiologic factors may be
considered under the heads of external and internal causes, or direct and
indirect.
As exemplifying the external causes may be mentioned the bites
or irritation produced by jelly-fish, mosquitos, fleas, stinging nettle,
certain kinds of caterpillars, bedbugs, etc. Constant scratching or any
persistent skin irritation, as in scabies and pediculosis, will at times
also be provocative. While, as a rule, in urticaria produced by this class
of etiologic factors the urticarial lesions appear only at the points or im
mediate neighborhood of the irritation, yet this is not always the case, as
in particularly susceptible individuals a general outbreak may result.
The internal or indirect causes are numerous, here again the indi
vidual peculiarity having a potent contributory influence. Most of this
class act through the stomach and intestinal tract. Among the more
common factors in this class may be mentioned oysters, clams, crabs,
lobsters, shrimps, mussels, fish, pork, more especially sausages and
scrapple, veal, nuts, mushrooms, strawberries, and cucumbers. In
addition to the articles of food named, others may be causative in special
instances, owing to some striking idiosyncrasy, such, for instance, as
oatmeal and butter. The irritation from intestinal worms may also be
the cause in the urticarias of children. The malady is not infrequent in
immigrants during their first several months’ stay in our country, doubt
less due to the complete change of diet and mode of living. An attack
may also result from the ingestion of certain medicinal substances, more
especially copaiba, cubebs, chloral, turpentine, quinin, opium, the
iodids, and many of the coal-tar products. The use of antitoxins has
added another cause occasionally provocative.
Emotional or psychic causes, such as anger, fright, or sudden grief,
will sometimes excite an outbreak, more especially if occurring during
or directly after a meal, the process of digestion being apparently inter
fered with, possibly permitting the development of toxins. Urticaria
is at times observed in association with malaria, jaundice, albuminuria,
and diabetes mellitus. The not infrequent occurrence of the disease in
rheumatic and gouty individuals would point to these constitutional con
ditions as likewise predisposing. Functional and organic diseases of the
uterus may also be found to be the important underlying etiologic factors,
especially in the recurrent and chronic cases. Surgical operations, more
particularly upon the abdominal cavity, exceptionally appear to be of
causative influence. In fact, whatever gives rise to profound nervous
disturbance must be looked upon as of some import. My own impres
sion has been that these various factors act principally by the disturbing
influence they may have upon the act of digestion. Beyond question,
toxins from without or within—autointoxication—must in this, as in some
other diseases of the skin, especially erythema multiforme, be considered
as the most common cause of the outbreak. The action of nervous
184 INFLAMMATIONS
influence, direct or indirect, is shown by a case reported by Oliver,1
where the eruption was due to eye-strain, persisting or recurring when
a change in lenses was necessary. Ravitch2 believes disturbances of the
thyroid to be a factor of importance in chronic urticaria.
In the past several years biologic investigations have been thought
to point out as probably first indicated by Wolff-Eisner that urticaria
(and other toxic dermatoses) may be due to a hypersensitiveness to a
foreign albuminoid substance—the albumin not being sufficiently split
up by the intestinal juices, such products being absorbed into the cir
culation, and provoking an outbreak. A hypersensitive or anaphylactic
condition may be thus brought about which makes the individual acutely
responsive to even the smallest quantity of such toxic substances. The
faulty or imperfect preparation of this protein for safe absorption might
be directly or indirectly due to any of the various etiologic factors named.
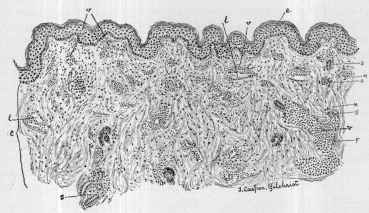
Fig 35-—Urticaria—section of a wheal: e, Epidermis, practically no alteration; c,
corium, showing acute inflammatory changes, swollen and infiltrated with serous exuda
tion, with the blood-vessels (v, v, v), especially those accompanying the sweat-ducts
(s, s, s, s) dilated and surrounded by and containing numerous polynuclear leukocytes;
lymphatic vessels (l, l) and spaces also enlarged, containing granular matter; numerous
mast-cells (m, m) scattered through the corium (courtesy of Dr. T. C. Gilchrist).
Pathology.—The pathology of urticaria is closely similar to that
of erythema multiforme. The disease is an angioneurosis, the lesions
being, primarily at least, due to vasomotor disturbance, which may be
of diverse origin, but doubtless most commonly toxinic; the angioneurotic
view has, however, some distinguished opponents. Barthélemy believes
dermatographism to be due to a toxic vasomotor dermatoneurosis.
In urticarial lesions dilatation following spasm of the vessels results in
effusion, and in consequence the overfilled vessels of the central por
tion are emptied by pressure of the exudation, and the pink or reddish
color gives place to central paleness, while the pressed back blood ac-
1 Oliver, Philadelphia Med. Jour., January 14, 1899.
2 Ravitch, “The Thyroid as a Factor in Urticaria Chronica,” Jour. Cutan. Dis.,
1907, p. 512; also Leopold-Levi and de Rothschild, Compt. rend. Soc. de Biol., Nov.,
1906.
URTICARIA
185
centuates the bright red tint of the periphery. Philippson,1 from animal
experiments, believes, with Heidenhain, that the secretion of lymph is
not a passive process due to intravascular pressure, as contended by
most dermatologists, but that a secretory action of the vascular endo-
thelium is involved; and that the edema of urticaria is similarly pro
duced by direct action of poisonous substances upon the vessels in the
neighborhood. Török and Hari's2 experimental studies are also in
accord with this view. Gilchrist's3 experimental observations led him
to a somewhat similar conclusion: that a true wheal is an acute, inflam
matory edematous swelling, due either to local inoculation of irritating
substances, as insect bites, etc, or to drugs or to some toxin probably
originating in the alimentary canal, the irritating agent producing death
of cells, which is followed by acute inflammatory changes. Wright and
Paramore4 believe that an attack of urticaria may be directly due to a
diminution of the lime salts in the blood, with consequent associated de
fective blood coagulability—is of the nature of a serous hemorrhage.
The pathologic anatomy of a wheal, studied by various observers
(Vidal, Unna, Gilchrist, and others), shows it to be a more or less firm
elevation of a circumscribed or somewhat diffused collection of semi-
fluid material, more especially in the upper layers of the skin. While it
has its usual seat in the derma proper, in intense cases the subcutaneous
tissue may also be involved in the process. Gilchrist found the epi
dermis unaltered, but the whole corium the seat of acute inflammatory
changes; the blood-vessels, especially those accompanying the sweat-
ducts, enlarged, containing and surrounded by a large number of poly-
nuclear leukocytes; the lymphatic vessels and the juice-spaces were
also much enlarged, containing only granular material; large numbers
of polynuclear cells were found to pervade the whole region, even into
the papillæ, but only a few had found their way into the epidermis.
There were numerous mast-cells throughout the corium, and the latter
was much swollen and infiltrated with serous exudation.
Diagnosis.—This rarely gives any difficulty. In fact, the disease
is so common and well known that the diagnosis is usually made by the
patient. The character of the lesions, their evanescent nature, the
irregular and general distribution, usually abundant upon covered parts,
and the accompanying intense itching, will afford sufficient basis for its
recognition. These points will serve to differentiate it from erythema
multiforme, to which it bears some resemblance. Urticaria bullosa
might, upon first and careless inspection, lead to a confusion with pem
phigus or dermatitis herpetiformis, but the usually preceding wheal
upon which the bleb arises, and the presence here and there of the ordi
nary type of the eruption, together with the history and course, will
prevent error.
1 Philippson, Giorn. ital., 1899, Fasc. vi, p. 675, abstract in Brit. Jour. Derm., 1900,
p. 217.
2 Török and Hari, “Experimentelle Untersuchungen über die Pathogenese der Urti
caria,” Archiv., 1903, vol. lxv, p. 21.
3 Gilchrist, “Some Experimental Observations on the Histopathology of Urticaria
Factitia,” Jour. Cutan. Dis., 1908, p. 122.
4Paramore (experimental study), Brit. Jour. Derm., 1906, pp. 239 and 248.
186
INFLAMMATIONS
Chronic urticaria has essentially the same features as the acute
disease, except the eruption is usually less abundant. It is not to be
forgotten that both pediculosis and scabies, as well as the irritation of
other animal parasites, may occasionally be responsible for scattered
wheals, but the other eruptive features of such maladies (q. v.) are usu
ally sufficiently distinctive to prevent confusion.
Prognosis.—The acute disease is of short duration, disappearing
spontaneously or as the result of treatment in several hours or a few
days; it may recur upon exposure to the exciting cause. Patients
with urticarial tendency should give special attention to the dietary,
and avoid those articles which may cause indigestion or which expe
rience has taught them may, owing to some idiosyncrasy, provoke
the disease. The prognosis of chronic urticaria is to be guarded, and
will depend upon the ability to discover and remove or modify the
etiologic factor. Recurrences are not uncommon.
Treatment.—Acute urticaria, the most common expression of
the disease, is usually due to stomach or digestive disturbance of acute
character. If the case is urgent and seen early, an emetic, to rid the
stomach quickly of the offending material, may be given; this is, however,
rarely required. The usual plan is to give a purge. For this purpose
there is nothing better than the antacid magnesia, although any of the
various salines will usually act satisfactorily. In addition to the purga
tive, an antacid should be administered at several hours’ interval, such
as sodium salicylate or sodium bicarbonate or benzoate; of the salicylate,
5 to io grains (0.35-0.65) three or four times daily, and of the others,
10 to 20 grains (0.65-1.35) at a dose; in children the doses should be
smaller. The diet for the time should be plain. In the vast majority
of the acute cases this simple plan of treatment will prove sufficient
to end the attack. If the attack should be somewhat persistent, the
alkali should be continued, and, in addition, small doses of salol and a
few grains of charcoal added to each dose. The calcined magnesia, too,
should be administered about every other night until the disease has
yielded.
It is, however, the chronic cases of urticaria which often tax our
therapeutic resources. Such cases require the most rigorous and care
ful examination, in order to discover, if possible, the underlying etiologic
factor or factors. The possibility of diabetes, albuminuria, disease of
the liver, and utero-ovarian disease being the influential cause should be
eliminated. The urine should be carefully and repeatedly examined,
for this sometimes gives the clue to the acting factor. Particular atten
tion should be given to the digestive apparatus, for probably this, as in
the acute cases, is the most common source of the disease. The patient‘s
habits as regards the use of alcohol and the use of drugs should also be
inquired into, as having a possible bearing.
There are many cases, it is true, of chronic urticaria in which the
etiology remains obscure, even after the most careful investigation,
and such cases must be treated empirically. Experience has taught
that the remedies most frequently successfully used in such cases are
quinin, sodium salicylate, atropin (Schwimmer and many others),
URTICARIA
187
pilocarpin (Pick), ergot, potassium bromid, salol, strophanthus (Riffat),
ichthyol, strychnin, calcium chlorid (Wright), along with saline laxa
tives. Arsenic may also be tried in resistant cases, although, except
indirectly, in small doses as a tonic, it is usually disappointing. The
most efficient of these in a given number of cases are atropin and sodium
salicylate.
Frequent and repeated doses of saline laxatives sometimes cure
when all the ordinary remedies have failed to make a permanent im
pression. For this purpose calcined magnesia, taken every second or
third night, or Carlsbad salts, magnesium sulphate, sodium sulphate,
Hunyadi Janos water, or Friedrichshall water, taken every morning
or every second morning, can be prescribed. The dose should be suffi
cient to produce free and prompt action, but not sufficiently large to bring
about a condition of diarrhea. The following also has given me satis
faction:
R. Sodii sulphat. granulat., 3ij (64.);
Sodii chlorid,, 3iiss (10.);
Sodii bicarbonat., 3vss (22.).
This should be kept in a closely stoppered, wide-mouthed bottle,
and one to two teaspoonfuls taken dissolved in a half to a tumblerful
of hot water twenty or thirty minutes before breakfast; or in some
cases it seems to act better when taken in smaller doses—a half to one
teaspoonful—before each meal. In obstinate cases spinal galvaniza
tion, static insulation, and the static current with the roller electrode
applied along the spine should be tried. Ravitch, in the belief that the
thyroid gland is a factor, has prescribed in atrophy and functional inac
tivity desiccated thyroid gland in chronic cases with alleged favorable
results; while in enlarged glands and hypersecretion such remedies as
thyroidectin, strophanthus, bromids, atropin, and x-ray.
It is understood that in all these cases the diet is to be carefully regu
lated, and all indigestible foods interdicted, and especially those articles
which experience has taught are not infrequently causative factors.
Coffee and tea in excess should also be avoided; in fact, these drinks
should be, in rebellious cases, forbidden absolutely. Resorting for a
time to an exclusively milk diet will sometimes prove curative, or at
least remove the disease for a time. In persistent cases of the disease
which have proved rebellious to all plans, especially those dependent
upon neurasthenic conditions, change of scene and climate will some
times give temporary, and not infrequently permanent, freedom.
If the eruption is extensive the itching is likely to be so trouble
some a feature that the patient loses much sleep, and in such instances,
occasionally, recourse must be had to potassium bromid, chloral, sul-
phonal, acetanilid, phenacetin, and the like. In a few instances two or
three daily doses of acetanilid or phenacetin in moderate quantity have,
as already intimated, afforded more or less permanent relief. Opiates
are usually to be avoided, inasmuch as they often increase the subjective
symptoms.
In most cases of urticaria it is found necessary to resort to local
applications to give some relief to the intense itching and burning which
188
INFLAMMATIONS
usually characterize the malady. The most efficient are those remedies
which are known to have an antipruritic action. Carbolic acid in
lotion form is one of the most valuable antipruritics in our possession.
It may be prescribed as in the following:
R. Acid, carbolici, 3ss-3j (2.-4.);
Glycerini, 3ss (2.);
Alcoholis, 3j (32.);
Aquæ, q. s. ad 3viij (256.).
Liquor carbonis detergens is another valuable preparation, and
may be used in the strength of 1 to 2 or 3 ounces (32. to 96.) to the
pint (500.) of water. A lotion of thymol, such as the following, will like
wise be found of value:
R. Thymolis, gr. viiss-xv (0.5-1.);
Glycerini, 3ij (8.);
Alcoholis, 3ij (64.);
Liquor potassæ, 3j (4.);
Aquæ, q. s. ad 3viij (256.).
Alkaline baths are also of great benefit in some cases. These may
be made with borax, sodium carbonate, sodium bicarbonate, 1 to 4
ounces (32. to 128.) to the bath of about 30 gallons; ammonium muriate,
1 to 2 ounces (32. to 64.) to the bath, is also useful. The patient should
remain in the bath from several minutes to ten or fifteen minutes, and
the temperature should be sufficiently warm that chilliness does not occur.
In mild cases, and even in some of the more severe cases, the use of a
dusting-powder on the affected surfaces will be sufficiently soothing, and
has the advantage of cleanliness and ease of application. For this pur
pose any of the ordinary dusting-powders, such as zinc oxid, rice flour,
talc, and boric acid, can be used.
Ointments are rarely of service in the ordinary type of this disease,
but in the types described as the vesicular and bullous varieties they
may be demanded for their soothing and protective influence. For
this purpose the plain zinc oxid ointment, with 5 or 10 grains (0.35 or
0.65) of resorcin or carbolic acid to the ounce (32.), will prove satis
factory. A boric acid ointment—1 dram (4.) of boric acid to the ounce
(32.) of cold cream—may also be of use. If there is a good deal of
irritation, the calamin-zinc-oxid lotion may likewise be employed in
these cases.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |