| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
REGIONAL AND INFANTILE ECZEMA
Regional and infantile eczemas are here considered mainly from
the standpoint of treatment. They differ in no material respects from
the disease, and its types as already described; if there is any modifi
cation, it will be referred to. Infantile eczema is usually of the acute
and subacute grades, for which the treatment is the same as that for
eczema of adults of the same types; mild remedies are, as a rule, how
ever, to be employed, and if the more stimulating applications are seem
ingly required to reach a result, they must be used with greater caution.
Overfeeding is occasionally a factor, though not so frequently as improper
and deficient supply. Bohn2 places a great deal of stress, and rightly, I
believe, upon obesity (Fettsucht) as a factor in infantile eczema in the
first and second years, due to the character and the often unnecessary
quantity of the nourishment given. The influence of digestion as an
important etiologic factor in infants,3 as well as in adults, must be borne
in mind, and proper feeding is, therefore, imperative.
1 Liquor picis alkalinus is made of 1 part caustic potash, 2 parts pix liquids, and
5 parts water; the potash is dissolved in the water and gradually added to the tar with
rubbing in a mortar.
2 Bohn, “Eczema,” p. 133, in Gerhardt's Handbuch der Kinderkrankheiten (Nach-
trag), Tübingen, 1883.
3 Schwartz, “Dermatoses liées aux troubles gastro-intestinaux chez les enfánts,”
These de Paris, 1892; A. J. Hall, “An Inquiry into the Ætiology of Infantile Eczema,”
Brit. Jour. Derm., 1905, pp. 161, 203, 241, and 287, and 1907, p. 4, gives a full review
and discussion of the subject with résumé of the opinions of other writers with conclu
sions unfavorable to the digestive disturbance theory. Towle and Talbot‘s investiga
tions (“Infantile Eczema and Indigestion,” Amer. Jour. Dis. Children, Oct., 1912, p.
219) indicate that it may have a contributing influence.
REGIONAL AND INFANTILE ECZEMA 315
In the following remarks on the regional forms but little will be
said as to diagnosis, etc, as such matters have already been fully con
sidered, and to Which the reader is referred for further information on
these points. The generally accepted plan of discussing the external
therapeutics of regional eczemas is, indeed, in great measure at least,
scarcely necessary if the principles of treatment are kept in mind; for
the selection of the remedial applications or plans of treatment is to be
based, irrespective of locality involved, almost wholly upon the char
acter and grade of the inflammatory process, remembering that those of
the acute type and many of the subacute type require soothing and
protective applications, while those of a sluggish infiltrated type usually
require stimulating applications. To a slight extent, it is true, region

Fig. 64.—Eczema of erythematosquamous and squamous variety, with considerable in
filtration; of long duration.
does sometimes influence the first choice of remedy and the method of
application, and for such reason a brief consideration of the various
regional eczemas can probably be profitably added to the directions al
ready given. Reference will also be made, when deemed necessary, to
those remedies most frequently employed in children.
Eczema of the Scalp (Eczema Capitis).1—The disease in this region
is to be differentiated from seborrhea, psoriasis, pediculosus, favus,
and ringworm, chiefly the first two. In the adult the most common
variety in this region is the erythematosquamous and squamous, and
1 The face and scalp are the most common sites for eczema in infants, often being
limited to a part or whole of either of these regions. Hall found in 100 cases of infantile
eczema the eruption first appeared on cheeks, forehead, or temples in 56, on scalp or ears
in 40, and elsewhere in 4.
316
INFLAMMATIONS
the inflammation, usually of the subacute and chronic grade. It fre
quently extends over the forehead and mastoid regions, in the latter
often to the back of the ears, presenting, especially in the fold, the
moist variety. In its management it is not necessary to sacrifice the
hair. If the scale accumulation is considerable, the free use of olive
or almond oil or liquid petrolatum, with 1 to 3 grains (0.065-0.2) of
resorcin or carbolic acid to the ounce (32.), is, for the first few days, ad
visable, followed by washing with a mild soap and water. This will
generally remove the accumulations, and often a continuance of this
plan, especially with a resorcin-containing oil, increasing this ingre
dient to 5 to 10 grains (0.33-0.65) to the ounce (32.), will lead to marked
improvement. After the scales have been removed, washing is repeated
only as demanded by cleanliness and scale reaccumulation—on the
average, about once every one or two weeks. In irritable cases this can
be dispensed with entirely and the parts cleansed by gentle rubbing with
the oil. A 2 to 4 per cent, ointment of salicylic acid, with 5 to 20 grains
(0.33-1.35) of resorcin to the ounce (32.), is often extremely useful in
these cases. In irritable cases in which there is but slight tendency to
scale formation, the application of a boric acid solution followed by a plain
salve, such as cold cream or petrolatum, can be used satisfactorily for a
time. Later, slightly or moderately stimulating ointment applications
are demanded, and among these the best are those of liquor carbonis
detergens, white precipitate, and calomel, at first weak, later stronger.
In thickened, infiltrated, obstinate cases oil of cade, with 1 to 3 parts of
olive oil or in ointment, is valuable; but in private practice it is quite fre
quently found objectionable on account of the penetrating tar odor.
B-naphthol ointment, 1 to 3 per cent, strength, can be used as a sub
stitute, and sometimes satisfactorily, but it at times proves irritating.
In the stubborn, infiltrated disease sometimes observed on the lower
occipital region verging on to the neck, the tar and calomel preparations
are satisfactory, but must often be used quite strong.
In infants and children the vesicular and vesicopustular eruptions
are not uncommon, and are also occasionally met with in the adult;
there is sometimes a good deal of crusting. If present, this is to be
removed in the manner already described above, or if abundant and ad
herent, as described in the preliminary general remarks concerning ex
ternal treatment. Salicylic acid ointments are useful in such cases, and
also white precipitate and alumnol ointments—of the first, 3 to 10
or more grains (0.2-0.65) and of the latter, 15 to 30 (1.-2.) grains to the
ounce (32.). When possible and feasible, the application of the mild
boric acid wash can advantageously be used with it. In infants of little
hair or when it is short, the zinc oxid ointment and salicylated paste
can be employed, but, as a rule, both in children and adults, the powder-
containing salves are not practicable for the scalp or other hairy regions.
In children and female adults with a pustular eczematous condition of
the scalp, especially posteriorly, the possibility of the presence of pediculi
being the exciting factor should be borne in mind. Even if these para
sites are secondary to the eczema, a cure is not possible unless they are
removed.
REGIONAL AND INFANTILE ECZEMA 317
In irrtable types, both in the infants and adults, the temporary
use of the mixture of equal parts of almond oil and lime-water with
1 or 2 grains of carbolic acid or resorcin to the ounce (0.065-0.135 to
32.) can be employed temporarily. On the other hand, in extremely
obstinate and sluggish cases, a small quantity of precipitated sulphur,
10 to 40 grains to the ounce (o.65-2.65 to 32.), can be added to the tar
ointment or other selected ointment.
The best ointment base for the scalp is one of equal parts of petrolatum
and cold cream or petrolatum and lard, sometimes with the addition of
10 to 20 per cent, of lanolin; in sluggish cases, and sometimes in other
cases, petrolatum can be used alone.
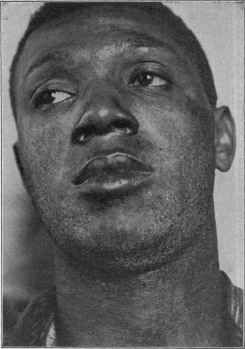
Fig. 65.—Eczema of erythematous and squamous variety in the negro.
Eczema of the Face (Eczema Faciei).—The disease in adults is to
be distinguished from seborrhea, dermatitis seborrhoica, dermatitis,
acne rosacea, and lupus erythematosus. The most common types are the
erythematous and erythematosquamous, but occasionally the papular
and, rarely, the pustular, and eczema rubrum, are also met with. An
erythematosquamous eczema of the forehead is sometimes observed,
in some instances of which the hatband is the exciting factor. Occa
sionally the erythematous variety limits itself to the lids and immediate
surrounding parts (eczema palpebrarum) or more frequently, it remains
here more obstinately after disappearing from other parts of the face.
Eczema of the lower part of the face, usually with upper part of the neck,
is occasionally due to the dye in fur boas, etc
318 INFLAMMATIONS
The various lines of treatment mentioned under the several inflam
matory grade headings are appropriately indicated here. The lotions
are especially useful, particularly the boric acid, calamin-and-zinc-oxid
lotions, and lotio nigra, the first or third conjointly with a salve, such
as cold cream, zinc oxid ointment, calamin-zinc-oxid ointment, and the
salicylated paste. For use on these parts white ointments can be
given a skin tinge by adding to the ounce several grains or more of
calamin, or a sufficient quantity of Armenian bole and umber (Brooke).1
Ointments can often be employed alone, but the conjoint use of especially
boric acid wash is often of added advantage. Cold cream is not only
soothing in itself in many of these cases, but it is also a satisfactory base
for other remedies. In the acute types the calamin-zinc-oxid lotion is
most efficient when applied by means of linen cloths, and kept constantly
wet with it; and in very irritable cases, instead of water, the basis of the
lotion can be made up of equal parts of lime-water and almond oil. Weak
ichthyol lotions, 1 to 10 per cent., are also useful. The liquor carbonis
detergens, both as wash and ointment, in the various strengths indi
cated, is often useful in the erythematous variety, and in the infiltrated
cases the stronger tarry ointments may be required, but here, as else
where, they should be applied tentatively at first. The bassorin, traga-
canth, and acacia paints are also useful in some cases. If the patient
is obliged to go out, the parts should be covered with a layer of grease to
protect from the air and wind; if the application being used is disfiguring,
at such times cold cream can be applied.
In infants and young children the vesicopapular, vesicopustular,
and eczema rubrum types are most common. It is to be distinguished
chiefly from impetigo contagiosa, miliaria, and less frequently dermatitis;
it could scarcely be confounded with lupus vulgaris. The mild applica
tions named should be always used in the beginning, and frequently ac
complish much, and sometimes lead on to cure; the conjoint treatment
with black wash and zinc ointment or boric acid lotion and zinc ointment
is often an admirable plan. The salicylated paste, with 3 to 10 grains of
carbolic acid to the ounce (0.2-0.65 to 3j), often, acts satisfactorily. In
some of the cases, and even when the condition looks quite actively in
flammatory, if considerably infiltrated, a tar-zinc-oxid ointment (tar
ointment, 3j (4.), zinc ointment, 3vij (28.)) brings about improvement,
and not infrequently quite rapidly; it should be tried on a small area at
first. Later, if the benefit flags, a larger proportion of tar can be added.
An important point in the care of some cases of eczema in infants is
the employment of mechanical restraint (White, Hall, Allen)2 to pre
vent rubbing and scratching, as by these latter not only is the appli
cation rubbed off, but the disease made worse; tying the hands loosely
to the lower part of the body or putting on loose mittens will serve
1 Brooke, “Mittheilung über eine Methode des Färbens von Salben,” Monatshefte,
1890, vol. xi, p. 62.
2 J. C. White, “Some of the Causes of Infantile Eczema, and the Importance of
Mechanical Restraint in Its Treatment,” Boston Med. and Surg. Jour., 1881, vol. cv, p.
365; H. J. Hall, “A Mechanical Treatment of the Eczema in Young Children,” ibid.,
1895, vol. cxxxii, p. 59; C. W. Allen, “The Treatment of Eczema in Infants and Chil
dren,'’ New York Med. Jour., 1899, vol. lxix, p. 433.
REGIONAL AND INFANTILE ECZEMA 319
to prevent. If these do not suffice, a pillow-case can be pulled over
the head, the closed end having had a hole sufficiently large cut in it
to permit the head going through; the open end is fastened around
the lower part of the body with safety-pins, and while the arms and
hands are somewhat free, the latter cannot be readily carried to the
face. In markedly itchy cases, both in children and adults, if the
remedies prescribed do not give some relief, or if so intense as to pre
vent sleep, carbolic acid, thymol, or resorcin should be added to the
applications named, in the quantity already stated in the general direc
tions for treatment. A short exposure to the Röntgen rays will some
times relieve the itching temporarily; and in obstinate cases of eczema
of these parts repeated exposures at intervals of several days may
have a curative influence. It is not, however, a method to be advised
in infants and children.
Eczema of the nares or nostrils (eczema narium) is sometimes seen
in young children as a pustular crusted eruption, often in conjunction
with a similar eruption about the corners of the mouth, simulating
closely impetigo contagiosa, except that it is chronic and persistent.
It is not infrequent also to see a slightly red, crusted condition of the
edge of the eyelids. It is most frequently seen in badly nourished stru-
mous subjects. The administration of cod-liver oil is often valuable
in these cases. Locally the best applications for the nose and corners
of the mouth are boric acid ointment, weak ointments (1 to 4 per
cent.) of calomel, and white precipitate.. For the edges of the lids
boric acid lotion, used freely and often, with boric acid ointment or a
1 to 2 per cent, yellow oxid of mercury ointment. The possibility
of an eczematous condition of edges of the lids being due to the pediculus
pubis is to be remembered, although such instances are rare. In adults
eczema of the nasal outlets is treated similarly. In these cases, as
also in those in children limited to the nares, a nasal catarrh is often
etiologic.
Eczema of the Ears (Eczema Aurium).—In some cases the eczema
is limited to the ears, often, more especially in children, to the poste
rior aspect and particularly in the crease, in which there is frequently
a tendency to oozing and fissuring. In this latter region the boric acid
lotion and the calamin-zinc-oxid ointment (calamin, 3j (4.)- zinc oxid
ointment, 3vij (28.)), and salicylated paste are usually most efficacious;
as the part becomes dry and scaly a small portion of tar, preferably,
at first, the liquor carbonis detergens, can be added to one of these
ointments, about 5 to 10 per cent, strength. In eczema of the auditory
canal the selected ointment should be free from any great proportion
of pulverulent substances; one of the salicylic acid, from 10 to 20 grains
(0.65-1.33) to the ounce (32.), or a 1 to 2 per cent, ointment of white
precipitate, calomel, or resorcin, answering the purpose best. It may be
gently applied with a piece of linen or small piece of cotton. An occasional
cleansing by gently wiping out the canal with almond oil, petrolatum, or
cold cream, and from time to time syringing the part with a solution of
boric acid containing \ to 2 grains (0.033-0.133) of borax to the ounce
(32.), will be found helpful.
320
INFLAMMATI0NS
Eczema of the Lips (Eczema Labiorum).—It is not uncommon to
see eczema limited to the lips and immediate adjacent parts. In these
cases the possibility of the tooth-wash or powder being an etiologic
factor (Neisser)1 should be eliminated. This has been the exciting
cause in several of my cases. Ehrmann2 has found eczema of the lips
usually in anemic individuals, the anemia promoting increased salivary
secretion, which acts as an irritant. The disease type may be either
the vesicopustular or erythematosquamous. It is frequently seen in
conjunction with the eruption on other parts of the face; exceptionally it
is confined to the upper lip and superjacent skin, and is attended with a
good deal of persistent swelling and infiltration. In the latter region
a nasal catarrh is sometimes the etiologic factor. A not infrequent fea
ture of lip cases is the tendency to fissuring.
In the moist crusted type the treatment is essentially that described
under eczema of the acute and subacute grades—boric acid and resorcin
lotions, with boric acid ointment, calamin-zinc-oxid ointment, and
weak white precipitate ointments. Later, when dry and the active
inflammatory character is reduced, the treatment can, if necessary be
changed to that of the erythematosquamous variety. In this latter,
however, it is well to begin as above, and then, if there is no positive
improvement, cautiously go to the tarry applications. The various
tragacanth, acacia, and gelatin paints are sometimes of value. Like
wise the zinc-oxid and boric-acid salve-mulls. In these cases, too, if
persistent, an occasional painting with a 2 to 5 per cent, silver nitrate
solution sometimes brings a result, although temporarily disfiguring.
Applying a paint of ol. cadini, 3ss-j (2.-4.); collodii, 3j (32.) (Hard-
away), is also an energetic measure that sometimes relieves. The
same may be said of frequent painting with benzoin tincture, with 5
to 10 grains (0.33-0.65) of boric acid to the ounce (32.). In using
these fixed applications the mouth should be gradually opened to its
widest capacity, and the lips then painted; if painted while closed
the dressing soon breaks, and the condition is often aggravated. The
Röntgen ray treatment is occasionally beneficial in lip eczema.
Eczema of the Bearded Region (Eczema Barbæ).—In other cases the
eruption is more or less confined to the bearded region, and is usually
of the papulopustular variety, of varying inflammatory grade. It is
rarely limited to the hairy region, but usually extends on to the bor
dering cheeks, and is often seen also in association with the eruption
elsewhere upon the face and body. Many of those cases in which it is
said to be confined to the bearded parts are in reality, I believe, cases
of sycosis vulgaris. There is, however, sometimes a close relationship.
In these patients the beard should be kept closely cropped, and when the
inflammation has measurably subsided, shaving is, as a rule, to be advised.
The applications are to be, at first at least, of the mildest character, and
preferably of lotions and ointments conjointly, and for the various plans
1 Neisser, “Lippen-Ekzem und Mundwässer,” Therapeutische Monatshefie, 1898,
vol. xii, p. 79; Galewsky, Mänch, med. Wochenschr., 1906, p. 1360.
2 Ehrmann, “Zur Aetiologie und Therapie des Mundwinkel- und Lippen-Ekzeme,”
Wien. med. Blätter, 1895, vol. xviii, p. 568.
Plate IX.

Eczema rubrum ; child eighteen months old ; duration one year ; considerable thickening,
gummy oozing, and crusting.
REGIONAL AND INFANTILE ECZEMA
321
advisable the reader is referred to the general directions concerning treat
ment already given.
Eczema of the Hands (Eczema Manuum).—The hands and especially
about the fingers are extremely common sites for the disease; the types
usually observed are the vesicular, the papulovesicular, and the scaly and
fissured. Fissures in these cases are quite frequent. A moist, usually
symmetric eczema of one or more of the interdigital spaces, but usually
that between the second and third fingers, and the immediately adjacent
parts,1 is not uncommon. The diagnosis is rarely difficult, as almost all
itchy eruptions of any chronicity, limited to the hand or hands and
the neighboring forearms, are eczematous. Occasionally, however, a
patchy vesicopapular or vesicobullous ringworm, sometimes rather acute
and more or less diffused, may simulate eczema very closely. The
disease is to be distinguished chiefly from dermatitis venenata and
pompholyx. In many of these cases the patient‘s occupation is the
exciting factor, and very often not much can be done in a permanent
way unless this is modified or suspended. In domestics who are obliged
to have their hands in water a great deal, loose rubber gloves should be
worn at such times. In all cases the hands should be protected from
cold and wind by the use of gloves.
In the moist types the conjoint use of black wash and zinc oxid
ointment is often serviceable; so is the use of a boric acid wash or a
resorcin wash, with the supplementary use of an ointment. The wash
should be dabbed on thoroughly, allowed to dry in, and then a small
quantity of the salve smeared over, or preferably applied spread upon
linen or lint. Used in this manner a well-made diachylon ointment
is often extremely valuable. The various mild ointments, without the
wash, are also beneficial at times. In the moist types, salicylated paste
is often an admirable application in this region. So also is the compound
stiff ointment plaster, consisting of equal parts of lead-plaster, soap-plas
ter, and petrolatum, with 10 grains (0.65) of salicylic acid to the ounce
(32.), spread upon linen or lint and closely adapted to the parts; with, if
there is much thickening, a larger quantity of salicylic acid—up to 1
dram (4.). In cold weather it is necessary to increase the proportion of
petrolatum. While the hands should ordinarily be washed as infrequently
as possible, owing to the damaging effects of soap and water, in thickened
and infiltrated cases a thorough washing with sapo viridis and hot water
nightly or every second or third night, according to circumstances, fol
lowed immediately by a mild salve application spread as a plaster, is often
of great therapeutic value.
For the dry, thickened types, especially observed on the palmar
aspects (eczema palmarum), one of the best remedies is salicylic acid,
applied as an ointment with petrolatum and benzoated lard as a base,
20 to 80 grains (1.33-5.33) to the ounce (32.); it should be well worked
in, and then applied as a spread-plaster. Occasionally an addition of
10 to 20 per cent, of lanolin to the base proves of advantage. Calo
mel and white precipitate ointments, usually strong, are likewise useful.
1 Dubreuilh, Annales, Dec, 1899, and Ciarrocchi, Trans, of Italian Dermatolog.
Soc'y for 1907, have called particular attention to this variety.
21
322
INFLAMNATIONS
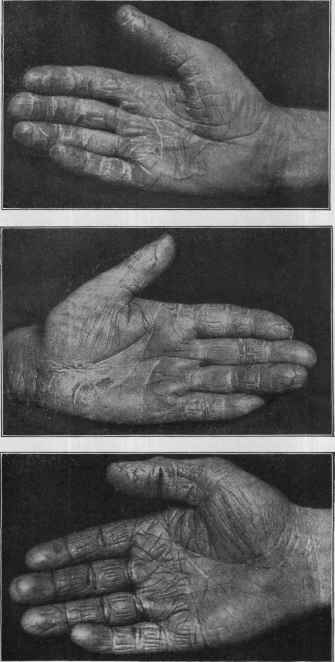
Figs. 66, 67, and 68.—Chronic squamous and fissured eczema of palms and fingers—
of various degrees and characters or types.
REGIONAL AND INFANTILE ECZEMA
323
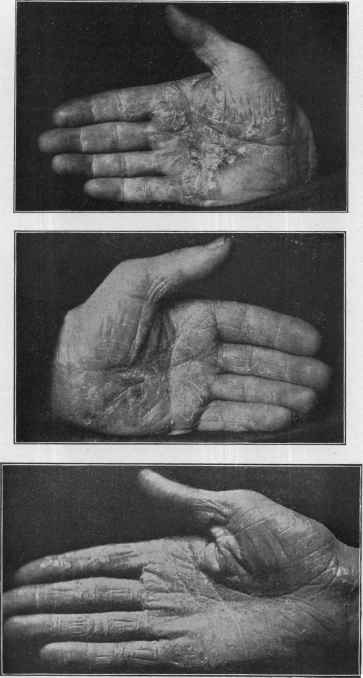
Figs. 69, 70, and 71.—Chronic squamous and fissured eczema of palms and fingers
—of various degrees, characters, or types; with considerable thickening; last is of sebor-
rheic type.
324
INFLAMMATIONS
Tarry preparations, in ointment form, are sometimes of distinct service,
but their action is doubtful in a given case, and they must be experiment
ally tried on a small surface at first. When there is marked epidermic
thickening, applications of the 10 to 25 per cent, salicylic acid rubber
plaster or plaster-mulls is applicable, and, as a rule, soon thin down the
parts. The same can sometimes be accomplished by painting on sali-
cylated collodion, 4 to 10 per cent, strength; after thorough washing, two
or three coats are painted on for two or three days, twice daily, and then
allowed to loosen; it is then repeated, if necessary, continuously or from
time to time. For the thickened palmar types Röntgen ray exposures
occasionally act admirably.
In chapping, the mildest example of fissured eczema, or at least a
condition allied thereto, a weak glycerin lotion or a mild ointment may
be rubbed in nightly; the hands should be kept out of water as much as
possible and, when washed, rubbed thoroughly dry. A good formula for
these cases is: R. Tinct. benzoin, co., 3ss (2.); glycerin, 5iiss (10.); alco-
holis, 3iij (52.); mix.
In eczema of the nails (eczema unguium) the nail involvement or
changes are usually due to eczema of the periungeal region. The in
volved nails should be closely filed or cut. The ordinary remedies in
the form of ointments can be applied, boric acid, salicylic acid, resorcin,
and ichthyol being the best. In obstinate cases painting every few days
with a 3 to 10 per cent, aqueous solution of silver nitrate or a saturated
solution in sweet spirits of niter is often successful; between the paintings
one of the above ointments can be kept applied.
Eczema of the feet (eczema pedum) demands no special directions;
that on the soles (eczema plantarum), in which there is usually marked
epidermic thickening, the treatment already outlined for the palms is
appropriate; exceptionally one of the fungi of ringworn (q. v.) has been
found in plantar epidermic thickening.
Eczema of the toes may be a part of an eczema involving more or
less of the feet, or it may not infrequently exist independently. While
all the toes may be affected, the outer three, as Jamieson pointed out,
seem more prone to the disease. The interdigital spaces are usually
especially involved, particularly primarily; developing slowly and
usually beginning as an insignificant repeated peeling of the skin, there
follow, sooner or later, maceration, redness, scaliness, fissuring, and
sometimes oozing, with variable thickening. It generally, after some
time, extends on to plantar and dorsal surfaces of the toes, and may
spread slightly, rarely extensively, up the foot. It is not to be over
looked that in some cases presenting the symptoms outlined instead of
a true eczema the malady is an anomalous ringworm (q. v.). For this re
gion, in addition to the milder applications, the occasional (every seven to
ten days) painting with a saturated solution of silver nitrate in spiritus
ætheris nitrosi, or as a 5 to 10 per cent, aqueous solution, or, cautiously,
with a 5 to 25 per cent, alcoholic solution of resorcin, is often especially
valuable. Ruggles1 commends, for the milder cases in which fissur-
ing is not a prominent feature, painting on once or twice daily an
1 Ruggles, “Eczema of the Toes,” Jour. Cutan. Dis., 1909, p. 105.
REGIONAL AND INFANTILE ECZEMA
325
alcoholic solution of 10 per cent, of tannic acid and 2 per cent, salicylic
acid.
Eczema of the Flexures (Eczema Articulorum; Eczema Intertrigo).—
Eczema of these parts is usually either erythematous or vesiculopapular,
sometimes with a resulting maceration of the surfaces, simulating ery
thema intertrigo, and in others developing into eczema rubrum. A
tendency to fissuring is not uncommon. As a rule, the conjoint use of
lotions and ointments yields the most rapid results. The boric acid
lotion and the zinc oxid ointment, or the salicylic acid paste, should be
used at first. The calamin-zinc-oxid lotion often acts well for several
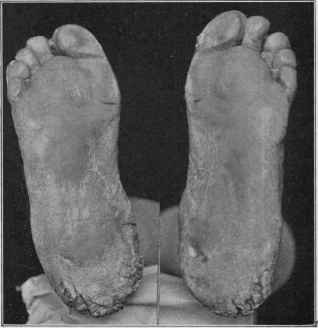
Fig. 72.—Eczema of a squamous, thickened, sclerous type, of about a year's dura
tion, in a woman aged fifty. Marked infiltration and callous formation about the
heels, with deep, painful fissuring; between some of the toes the eruption was of a mild
erythematous type, occasionally moist and oozing. In places there was a strong re
semblance to callositas.
days, but it is apt to be too drying unless intermitted and a salve employed
for a day or two. It can generally be continued longer if glycerin is
added, 5 to 15 minims (0.33-1.) to the ounce (32.). The boric acid and
the zinc oxid salve-mulls are extremely serviceable; also, for a time, if
any infiltration, the salicylated soap-plaster. Eczema under the breasts
in women is similarly treated. In this region, as well as in others where
parts come in contact, the wearing of flattened thin cheese-cloth bags
filled with a dusting-powder is often of great service. Later, if no bene
fit ensues or as soon as the good effects of mild treatment begin to flag, an
ointment containing varying quantities of white precipitate or calomel;
or the zinc oxid ointment, with 1 or 2 drams (4.-8.) of tar ointment to the
326 INFLAMMATIONS
ounce (32.); and in thickened, infiltrated cases tar ointment itself,
weakened at first, often proves of marked advantage.
Eczema of the Breasts (Eczema Mammæ seu Mammarum) and of the
Umbilicus (Eczema Umbilici).—Eczema of the nipple and immediate
surrounding skin in women is most commonly observed during the
nursing period, and may be of the dry or moist type, more frequently
the latter. In some subjects the condition is scarcely eczematous,
and presents merely fissuring of the nipples, the skin of the same being
dry and inelastic. The disease in this region is to be distinguished
from Paget‘s disease (q. v.). The mild plans of treatment will be found
most serviceable, those designated in the general directions as suitable

Fig. 73.—Eczema rubrum, of considerable duration, involving scrotum chiefly,
together with part of the shaft of the penis and adjacent portion of the thighs; marked
thickening and crusting (courtesy of Dr. M. B. Hartzell).
for the acutely inflammatory type of the disease; ordinarily a nipple-
shield should be worn at the time of nursing. In some cases, especially
when more or less confined to the nipples, with fissuring, painting the
parts with benzoin tincture, compound benzoin tincture, or with collodion
will tend to heal the fissures and improve the disease, and, at the same
time, measurably afford protection during the act of nursing. In ob
stinate fissures touching gently with silver nitrate or with the saturated
solution of silver nitrate in spiritus ætheris nitrosi can be tried, and often
proves effective. In eczema of the umbilicus the same mild measures
are usually successful, along with frequent washing with boric acid lotion.
In persistent cases the above solution of silver nitrate can be used.
REGIONAL AND INFANTILE ECZEMA 327
Eczema of the Genital Region (Eczema Genitalium).—The disease
about these parts is usually of the erythematous variety, although the
erythematopapular and erythematosquamous are not uncommon, and,
in fact, any type may exist. It is to be distinguished from eczema
marginatum (tinea cruris), dermatitis seborrhoica, pediculosis pubis,
and pruritus. Itching is often severe and a tendency to fissuring is not
uncommon. Glycosuria is to be excluded as a factor, especially in women.
In males the eruption is often confined to the scrotum, and more especially
to those parts coming in contact with the thighs; it may, however, be
quite extensive, involving shaft, glans, and neighboring parts of thighs
and perineum. In women the labia are usually the seat of the malady,
occasionally extending on to the mucous membrane; in some cases there
is moist exudation. Eczema of the vulva is sometimes provoked or
kept up by the use of certain irritating toilet papers women are apt to
use for drying the parts after urination.
The treatment differs in no way from that of the disease elsewhere,
but, owing to the heat, friction, and moisture of the parts, the condi
tion is usually extremely rebellious. Lotions of calamin-zinc-oxid,
of resorcin, liquor carbonis detergens, boric acid, and ointments of
calomel, calamin, the salicylic acid paste, zinc oxid and boric acid salve-
mulls, and, later, ointments of tar, may be used. The scrotum should
be supported by a suspensory bag as high as possible, so as to keep the
surfaces from contact. Sometimes this latter is best accomplished by
the use of flat cheese-cloth bags containing dusting-powder, by means
of which the parts can be kept separated. In obstinate cases the oint
ments may be applied spread on lint or linen and kept in place by means
of a bandage. In stubborn cases a medicated paint of tincture of benzoin,
with a few grains of salicylic acid or 20 to 30 grains (1.33-2.) of boric acid,
or ½ to 1 dram (2.-4.) of oil of cade to the ounce (32.), may be cautiously
tried. A frequently successful plan or adjuvant measure is the applica
tion, in scant quantity, of a 2 to 3 per cent, solution of silver nitrate in
spiritus ætheris nitrosi; it causes variable smarting momentarily. It is
repeated about once weekly, and mild salves used in the interval. In
women similar measures are employed. In addition to saccharine urine
being an occasional cause, irritating vaginal discharges are also sometimes
etiologic. In both sexes an occasional cleansing with hot boric acid solu
tion with ½ to 2 grains (0.033-0.133) of borax to the ounce (32.) is neces
sary; such application, if very hot, will also often allay the itching.
Soap and water should be used but seldom.
Eczema of the Anal Region (Eczema Ani).—Eczema of the anus is,
as a rule, a most intractable disease, and for evident reasons. It is to
be distinguished from pruritus. Seat-worms, hemorrhoids, fissure,
and fistula should be eliminated as causes. Exceptionally the use of
certain irritating toilet papers may provoke or keep the disease up.
After each stool the part should be gently cleansed and the remedial
application made. The application should be repeated again at the end
of eight or ten hours, without the preliminary washing. If moderately
or markedly inflammatory, the various mild lotions and ointments, such
as named for eczema of the genitals, should be at first employed; as a rule,
328
INFLAMMATIONS
however, these cases are sluggishly inflammatory and bear strong reme
dies. An ointment of liquor carbonis detergens, from 1 to 2 drams
(4.-8.) to the ounce (32.) of simple cerate or prepared suet, is espe
cially useful in some of these cases. Resorcin lotion, followed by a
mild ointment, forms also a good plan of treatment. Tar ointment,
weakened or of full strength, or a 10 to 20 per cent, ointment of oil
of cade, is also valuable in some instances. The oil of cade is often
serviceable, too, when used with almond or olive oil. In the applica
tion of these preparations the excess can be wiped off, and a dusting-
powder used to prevent soiling. In this region very frequently all
the various applications will be tried before permanent relief is brought
about. For the intense itching sometimes present in eczema of this
region applications of water as hot as can be borne may be used, often
with prompt relief, and the boric acid solution containing borax, as ad
vised in Eczema genitalium, can also often be used here with advantage.
Carbolic acid lotions, thymol lotions, and the application of liquid petro
latum, containing from 5 to 20 grains (0.33-1.33) of menthol or from 2 to
5 grains (0.13-0.33) of cocain to the ounce (32.), will allay the itching in
some cases, and also exhibit curative effects. A 5 to 15 per cent, calomel
cold cream sometimes acts surprisingly well. The Röntgen-ray treat
ment is sometimes valuable.
Eczema of the Legs (Eczema Crurum; Eczema Cruraie).—The legs
are quite commonly the site for eczema in those of middle life and
advancing years. The condition is more or less complicated by the
fact that the circulation is less active in dependent parts; varicose
veins are not infrequently associated, and in some instances may exist
for months or years before the eczema (eczema varicosum) develops,
having in many cases an undoubtedly causative influence. The type
of disease most common in this region is eczema rubrum, and not in
frequently the erythematosquamous and squamous; on the lower part,
in the region of the ankle, often extending on to the foot, the thickened,
scaly, sclerous, and verrucous forms are usually observed. There
is occasionally noted also a mild, persistent, erythematous type, with
but little if any tendency to scale-formation, in which here and there,
few or in crowded number, minute hemorrhagic puncta are noted;
sometimes this purpura-like feature is of more or less diffused character
over the affected area or region.1 The treatment of ordinary eczema
rubrum of the leg differs very little from that of other parts. Mild
applications should be used at first, such as boric acid lotion, black wash,
or a resorcin lotion, followed by salicylic acid paste, zinc oxid ointment,
calamin ointment, or the stiff salicylated plaster-like ointment already
referred to. The ointment should be spread upon lint or any suitable
material, and applied as a plaster, being closely adapted to the parts.
In some cases the free use of the calamin-zinc-oxid lotion will rapidly
change the case into a dry type. Occasional washing is necessary, the
best plan being to wipe off gently any ointment that may have collected,
and to soak the part in a bucket of warm water made alkaline by the addi-
1 See interesting paper by Klotz, “Dermatitis Hæmostatica,” Jour. Cutan. Dis.,
1891, p. 361; and by Schamberg, Brit. Jour. Derm., 1901, p. 1.
REGIONAL AND INFANTILE ECZEMA 329
tion of from 1 to 4 drams (4.-16.) of borax or sodium bicarbonate; after
withdrawing the part it is to be again gently wiped and tapped (not
rubbed) dry and the remedial application again made. After the diseased
area has lost its moist character the ointment may be made slightly
stimulating by the addition of from 10 to 30 grains (0.65-2.) of white
precipitate or calomel to the ounce (32.); later, in addition to its applica
tion as a plaster, a small portion of the salve may be gently rubbed
into the skin of the affected area; or this latter plan of rubbing in
may of itself, in the dry types, be sufficient. Stronger remedies
may be gradually used if the improvement flags, and a weak tarry
ointment may be eventually employed in many of these cases with
great advantage.
In eczema rubrum with much thickening, and when the irritability
is not great, vigorous shampooing with hot water and sapo viridis may
be practised every few days, even to the extent of producing a good deal
of temporary disturbance; then rinsing and drying the part and imme
diately applying a mild salve spread as a plaster. This plan will oc
casionally act with surprisingly favorable effect upon the disease. In
dry eczemas of the leg ointments containing varying proportions of
salicylic acid, tar, calomel, and other stimulating remedies may be
rubbed in twice daily; and in these the application of the salve as a
plaster is not, as a rule, necessary. A most satisfactory plan of treat
ment in the majority of cases is that by the gelatin dressing, already
described in the general section on the treatment of eczema in discussing
the remedies applicable to the subacute variety; this finds its best
application when the disease is dry, but it may also be used in the moist
type so soon as its moist character has measurably been controlled.
The parts should be free from scales or crusts before applying.
The purely medical treatment of eczema of this part may, especially
in those in whom a varicose condition of the veins seems predisposing
or causative, be considerably aided by giving support to the leg by
means of a properly applied roller-bandage or by a gum stocking. The
gelatin dressing referred to does this, and this is one of its advantages.
The rubber bandage will prove useful in a few cases, but if applied directly
over the parts it is likely to irritate, so that a thin layer of bandage
should be placed next to the skin. In ordinary cases the support to the
part need be given only during the day, when the patient is for most of
the time in the upright position; during the night it is not necessary,
except in markedly varicose conditions. As a rule, however, neither
gum stocking nor rubber bandage is so satisfactory during the treatment
as the roller-bandage; and in my experience the rubber bandage is so often
disappointing and even aggravating in its effects that it has been practi
cally discarded. The cotton elastic bandage, however, can satisfactorily
take its place.
In eczema of the leg complicated by an ulcer this latter is to be
treated in the ordinary manner,—“strapping” is, however, as a rule,
not permissible; an excellent method in these cases is by the gelatin
dressing, leaving an opening over the ulcer, and treating this by the
usual applications.
33°
INFLAMMATIONS
The sclerous, verrucous types are to be treated as already referred
to in the general directions.
Generalized or Universal Eczema (Eczema Universale).—This term
is usually applied, as has been already stated, to eczema involving
the whole or greater part of the surface; it is often more or less acute
in character. Universal eczema, strictly speaking, is, however, rare.
The erythematous and mild scaly types are most common; eczema
rubrum, more or less generalized, has also been observed; in fact, any
type may exist, and in some instances there is only a preponderance
of one type, the disease upon different parts presenting different aspects.
In these cases the patient is most comfortable in bed, at least until the
activity of the inflammation has abated. Lotions and dusting-powders
used conjointly are most comforting in dry eczema, while in moist eczema
lotions and ointments usually furnish the most relief. There is, however,
no set rule for this. The remedies should not be strong. These cases
generally do well at first, the disease frequently yielding rapidly, except
upon one or more regions, where it is likely to persist for some time. The
type (eczema craquelé) of more or less generalized eczema sometimes
met with, in which there is practically but little, if any, infiltration of the
skin, being erythematous and in places minutely vesicopapular, and
tending to crack superficially in irregular squares or blocks, has already
been referred to in the description of the varieties. This variety requires
the mildest kind of treatment, the salicylic acid paste, plain salicylated
petrolatum, 5 grains (0.33) to the ounce (32.), and petrolatum or cold
cream, containing 1 or 2 drams (4.-8.) of powdered starch to the ounce
(32.), acting most satisfactorily.
Eczema of the Adjoining Mucous Surfaces.1—The mucous membrane
is rarely, if ever, solely involved, but in conjunction with the neigh
boring cutaneous surface, as at the nasal orifices, the eyelids, the lips,
about the glans penis, the vulvar orifice, and the anus. The membrane
becomes inflamed and somewhat thickened, sometimes dryer than nor
mal, and at other times showing a mucopurulent discharge. Crusting,
usually insignificant, may at times form, and occasionally there is a
slight disposition to crack. Exceptionally the disease is limited to
the vermilion of the lips, and is persistent, but this, I believe, belongs
to the domain of dermatitis seborrhoica and will be again referred to
under that head. The benign evanescent plaques sometimes observed
on the tongue will be referred to elsewhere.
Its continuity from the disease of the cutaneous surface, from which
it usually springs, would suggest a parasitic factor. At times, especially
about the nose and mouth, it would almost seem as if it had its com
mencement on the mucous surface, certainly at least at the mucocuta-
neous junction. In the treatment of the disease on these parts measures
vary somewhat as to locality. That of the nares has already been
spoken of, as well as that at the edges of the eyelids. For the glans
penis and the inner surface of the vulva, as well as, in fact, on all other
1 Vidal, Gazette des hôpitaux, 1880, p. 68; Besnier, Jour, de med. et de chirurg.,
Dec, 1889; von Sehlen, Monatshefte, 1894, xix, p. 15; Hartzell, Medical News, 1895,
i, p. 460 (with literature references).
DERMATITIS SEBORRHOICA
331
mucous surfaces, boric acid lotions and 1 to 5 per cent, tannic acid solu
tions are valuable; and in persistent cases the silver nitrate solutions
already referred to several times are to be kept in mind.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |