| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
PEMPHIGUS
Synonyms.—Fr., Pemphigus; Ger., Pemphigus; Blasenausschlag.
Definition.—Pemphigus is an acute or chronic bullous disease,
characterized by the formation of scanty or numerous irregularly
scattered, variously sized, rounded or oval blebs, arising from appar
ently normal or moderately reddened skin, and which may or may
not be accompanied by mild or severe constitutional disturbance.
Numerous so-called varieties of this rare and as yet obscure disease
have been described, based chiefly upon the duration, age of the patient,
and the clinical characters and behavior of the eruption. The division
is in many respects purely arbitrary. The whole subject of pemphigus
is, in fact, at present chaotic, and it is a matter of difficulty even to the
trained dermatologist to know what to include and what not to include
under this head. Many of the cases formerly considered in this class,
372
INFLAMMATIONS
and still so considered by some German writers, have been gathered
together to form the group constituting the dermatitis herpetiformis of
Duhring.1
The presence of a bleb or blebs does not, however, as often con
sidered by many physicians, constitute pemphigus, as such lesions are
often seen as an accidental or unusual manifestation in other diseases,
such, for example, in urticaria (urticaria bullosa), erythema multiforme
(erythema bullosum), dermatitis herpetiformis, just referred to, pom-
pholyx, dermatitis venenata, leprosy, and some others. On the con
trary, pemphigus is a malady in which the lesions consist, primarily at
least, of distinct watery rounded blebs, of more or less general distribu
tion, without ring or other peculiar formation or special tendency to
group, and appearing irregularly or in successive crops, and, as a rule,
running a chronic course, with exacerbations. The subjective symptoms
usually consist of tenderness, soreness, and burning, and less frequently
itching.
The varieties of pemphigus can be described under the heads of pem
phigus acutus, pemphigus chronicus, pemphigus foliaceus, and pemphigus
vegetans. The terms “benignus,” “malignus,” “gangrænosus,” “hæmor-
rhagicus,” etc, sometimes added to pemphigus, are self-explanatory.
The cases described under the headings “Pemphigus Contagiosus”
Pemphigus Neonatorum, Pemphigus Epidemicus, etc, while included,
really represent, I believe, extensive and grave types of impetigo con-
tagiosa.
Symptoms.—Pemphigus Acutus.2—Acute pemphigus includes all
1 Recent papers on the classification of bullous diseases by Bowen and by Bronson,
with discussion, are to be found in the Trans. Amer. Derm. Assoc. for 1905, and Jour.
Cutan. Dis., 1906, pp. 110-217, and by Corlett, ibid., 1906, p. 464 (an analysis of 65
bullous cases); Zeisler, “Pemphigus,” Jour. Amer. Med. Assoc, 1907, vol. xlix, p. 270
(with report of cases). Winfield, “Pemphigus and Bullous Dermatoses,” Jour. Cutan.
Dis., 1908, p. 566 (with bibliography); Macleod, ‘‘The Present State of Our Knowledge
of Pemphigus,” Practitioner, 1909, No. 82, p. 371; Pernet, “Pemphigus and Dermatitis
Herpetiformis,” Brit. Jour. Derm., Jan., 1910, reports a case of acute septic pem
phigus in a woman, followed after convalescence and recovery by an eruption of the
type of dermatitis herpetiformis; Hartzell, “Toxic Dermatoses; Dermatitis Herpeti-
formis, Pemphigus, and Some Other Bullous Affections of Uncertain Place,” Jour.
Cutan. Dis., 1912, p. 119; Brocq, Annales, Jan., 1912, p. 1, endeavors to simplify and
clarify the complicated subject of the classification of the bullous diseases.
2 Some literature on acute pemphigus: Pernet and Bulloch, “Acute Pemphigus: A
Contribution to the Etiology of the Bullous Eruptions,” Brit. Jour. Derm., 1896, pp.
157 and 205. This admirable paper refers to the various acute types, especially to that
in adults due to infection from animals or their products. The subject is presented in
its clinical, etiologic, bacteriologic, and histopathologic aspects—with numerous litera
ture references. The reader is referred to this paper for many references made in my
own text, especially as to bacteriologic findings. Hadley and Bulloch, Lancet, May 6,
1899 (fatal case in butcher, starting in finger injury); Ravogli, Cincinnati Lancet-
Clinic, April 27, 1889, p. 481; Schamberg, Annals of Gynecology and Pediatry, Feb.,
1901, p. 321 (fatal case, apparently due to vaccination); Whipham, Lancet, 1896, i, p.
1219 (2 cases; arsenic treatment, 1 death, 1 recovery; with some bacteriologic experi
ments by S. R. Wells); Robinson, Manual of Dermatology, p. 234; Rose, Montreal Med.
Jour., Jan., 1899, p. 50 (in the course of a fatal case of alcoholic delirium); Caie, Brit. Med.
Jour., 1903, vol. i, p. 308, a case of acute malignant pemphigus, ending fatally in twelve
days; the patient, a male adult, worked among cattle, and shortly before the erup
tion had pricked his hand while washing sheep; Howe, “Cases of Bullous Dermatitis
Following Vaccination,” Jour. Cutan. Dis., 1903, p. 254 (with several case illustrations;
a series of 10 cases, all, except 1, occurring in those recently vaccinated; 6 of these cases
died); Bowen, “Acute Infectious Pemphigus in a Butcher, During an Epizootic of
PEMPHIGUS 373
those cases in which the course is more or less limited, and the termi
nation, within several weeks or a few months, in recovery or death.
Its occurrence has been denied, but occasional observations, now con
siderable in number (Damon, Rayer, Cazenave, Neumann, Allen,
Payne, Behrend, Shillitoe, Roach, Van Harlingen, and others), leave
no doubt as to its existence. It is, however, rare, and seen for the most
part in children of early age, although it is also exceptionally seen in
the adult. It is occasionally observed (Hardy) in young girls between
the period of puberty and full sexual maturity with menstrual difficulties
(so-called pemphigus virginum, pemphigus hystericus). In its clear
type (blister fever, febris bullosa, pemphigus febrilis) the eruption
usually comes out suddenly, with premonitory symptoms of malaise,
slight or severe febrile action, chilliness or rigors, and other evidence of

Fig. 89.—Pemphigus in a negress aged thirty-one, of two months’ duration, showing
the fresh, tense, and older flaccid blebs on upper arm; eruption general. Irregular
febrile disturbance, but otherwise patient‘s health seemed good.
mild or grave systemic disturbance. The lesions are variously sized
from that of a pea to that of a pigeon's egg or larger, are generally quite
abundant, and irregularly distributed over the surface; they are dis-
Foot and Mouth Disease, with a Consideration of the Possible Relationship of the Two
Affections,” Jour. Cutan. Dis., 1904, p. 253 (reviews the subject of acute pemphigus,
especially as to its possible origin from animal sources, and gives a résumé of reported
cases with references); Saundby, Lancet, Oct. 1, 1904, reports a case of acute pem
phigus in a butcher‘s apprentice; Corlett‘s case, Jour. Cutan. Dis., 1908, p. 7, with
circinate and hemorrhagic bullous lesions, apparently due to streptococcic infection
and ending fatally, seems to me to belong here rather than in the group erythema mul-
tiforme as reported; Grindon, “Acute Septic Pemphigus,” ibid., 1900, p. 439 (death;
case illustration; patient had to do with cattle and other animals); Pollitzer, “A Fatal
Case of Bullous Dermatitis,” Jour. Cutan. Dis., 1911, p. 209— a male, aged fifty-six,
beginning as an intensely itchy erythrodermia, and later developing pemphigoid lesions,
and, soon after, profound toxemia; had been in good health except for a chronic diffuse
nephritis which had apparently given no trouble; death within six weeks; postmortem
and bacteriologic findings and experimental inoculations negative.
374 INFLAMMATIONS
tended or somewhat flattened, come out at one time or in rapid succession
or in distinct crops, and, as a rule, arise from skin showing no preliminary
change; sometimes, however, from a slightly hyperemic surface. Some
are usually surrounded by a narrow red halo. Generally clear at first,
they often become milky and opaque, sometimes hemorrhagic, and
exceptionally gangrenous. In other instances the eruption is unaccom
panied by pronounced constitutional involvement, and in others the
febrile action and other systemic symptoms of varied nature continue
for the first week or two, until subsidence of the cutaneous phenomena
sets in; in such instances complete recovery usually takes place in several
weeks to one or two months.
In some of the febrile cases grave symptoms present or continue
to increase in severity, the throat and mouth show serious involvement,
the blebs become flaccid and puriform, and exceptionally the under
lying surface, gangrenous (Lenhartz), and death follows in one to
several weeks. In some instances the disease, after the more acute
outbreaks have subsided, gradually becomes less active, the lesions
are less numerous, and it goes into the chronic form.
The blebs disappear, sometimes partly by absorption, with desic
cation and crusting, or sometimes purely by desiccation and crusting,
with or without previous accidental or spontaneous rupture; when
the crust falls off, slight temporary redness or staining is noted, but
there is no permanent trace left.
The acute type is usually observed as isolated cases, but it has, or
a disease simulating it, been observed (Colrat, Köhler, Bernstein, and
others) to occur in epidemic form (pemphigus epidemicus, pemphigus
contagiosus); in some instances with but slight constitutional symp
toms or entirely free from such, and in others moderately active and oc
casionally severe. These doubtless are similar to the contagious or
infectious cases observed in the newborn—pemphigus neonatorum
—to be referred to. It is highly probable that many of the reported
epidemic and contagious cases are examples of impetigo contagiosa
and bullous varicella. The benign pemphigus contagiosus described
by Manson as quite common in the tropics is probably a variety of
impetigo contagiosa; it is usually diffused in children, but in adults
chiefly about the axillary and genito-crural regions, and in the latter
sometimes representing doubtless “dhobie itch.”
Pemphigus Acutus Neonatorum1 (Pemphigus neonatorum; Pem-
1 Literature bearing upon pemphigus neonatorum, pemphigus epidemicus, and
pemphigus contagiosus: Staub, “Ueber den Pemphigus der neugeborenen und der
Wöcherinnen,” Bericht des II. Intemat, Dermatolog. Congress, 1892, p. 699; Strelitz,
“Bacteriologische Untersuchungen über den Pemphigus neonatorum,” Archiv für Kin
derheilkunde, 1890, vol. xi, p. 7; and 1893, vol. xv, p. 101; Peter, “Zur Aetiologie des
Pemphigus neonatorum,” Berlin klin. Wochenschr., 1896, p. 124 (in infant suckled by
septicemic mother); Zechmeister, “Ueber Pemphigus neonatorum,” Münchener med.
Wochenschr., 1887, p. 737—abstract in Archiv, 1888, p. 271 (in 76 births under charge
of one midwife 28 cases developed, of which 6 were fatal); Wichmann, “Epidemie von
Pemphigus Contagiosus,” Tidsskrift für praktisk Medicin, 1887, No. 21—abstract in
Archiv, 1888, p. 423 (in the newborn; 23 cases, of which 3 died—all the children born
under the care of the same midwife); Jükovsky, “Pemphigus neonatorum," Vratch,
No. 15, 1891, p. 357—abstract in Brit. Jour. Derm., 1891, p. 368 (12 infants, of which
4 died—all born under care of same midwife); Kilham, “An Epidemic of Pemphigus
PEMPHIGUS
375
phigus neonatorum contagiosus; Pemphigus epidemicus; Pemphigus
contagiosus).—The cases usually included under this subheading of
acute pemphigus, and formerly believed, and still believed by a few
observers, to represent a distinct pemphigus type, are those observed
a few days after birth, many of which run a short, mild course, others
going on to a rapidly fatal termination. Almost all, and probably
all, these cases, as Richter‘s analytical study and later observations
Neonatorum,” Amer. Jour, of Obstet., 1889, p. 1039 (12.cases, all mild; bacteriologic
examination negative); Homolle, “Epidemic of Acute Pemphigus in the New-born,”
Gazette Hebdom., Nov. 13, 1874—abstract in Arch. Derm., 1875, p. 154 (among 79
births but few escaped; the disease was mild, but 1 case ending fatally; inocu
lation experiments negative); Corlett, Indiana Med. Jour., Nov., 1893, p. 158;
Moldenhauer, “Ein Beitrag zur Lehre vom Pemphigus acutus,” Archiv für Gynäkol.,
1874, vol. vi, p. 369 (101 cases observed in a period of about a year—mild, and dis
tribution, character, and behavior indicate that they were cases of impetigo conta-
giosa); Klemm, “Zur Kenntniss des Pemphigus contagiosus,” Deutsches Archiv für
klin. Medicin, 1871, vol. ix, p. 199 (28 cases are reported, and a study of which leaves
but little doubt that they were examples of impetigo contagiosa); Faber, “Ueber den
acuten contagiösen Pemphigus,” Monatshefte, 1890, vol. x, p. 253 (an analytic paper
of reported cases, indicating the probability that many were impetigo contagiosa);
Greer, “Puerperal Septicemia and Pemphigus Neonatorum,” Brit. Med. Jour., 1894,
i, p. 1241; Holt, “Pemphigus Neonatorum” (1 case associated with general infection
with staphylococcus pyogenes; death), N. Y. Med. Jour., 1898, i, p. 175; Solbrig,
“Pemphigus neonatorum,” Zeitschrift für Med.-Beamte, 1900, vol. xiii, p. 41; Köhler,
“Ueber die Diagnose und Pathogenese akuter Blasenbildung der Haut nebst kasuis-
tischem Beitrag zur ‘Febris bullosa’" (small epidemic of 7 cases, 1 of which died),
Deutsches Archiv für klin. Medicin, 1899, vol. lxii, p. 579; Bernstein, “Ein Beitrag
zur Kenntniss des Pemphigus neonatorum acutus” (5 cases, infants and adult; some
what suggestive of impetigo contagiosa, although the reporter excludes this, and ex
perimental inoculations were negative), Monatshefte, 1899, vol. xxviii, p. 19; Bloch,
“Pemphigus neonatorum,” Archiv für Kinderheilk., 1900, vol. xxviii, p. 61 (an obser
vation of 20 cases, some fatal; clinical, anatomic, and bacteriologic aspects are pre
sented); Knocker, “Pemphigus Neonatorum” (2 cases, mild in type; had been de
livered and looked after by the same nurse), Brit. Jour. Derm., 1898, p. 195; Beck,
“Aetiologie des Pemphigus neonatorum” (1 case—death; cocci, usually paired, found
in lesions and blood)—abstract in Monatshefte, 1899, vol. xxviii, p. 410; Windisch,
“Pemphigus Contagiosus Tropicus,” Jour. Amer. Med. Assoc, 1900, vol. xxxiv, p. 77;
Munro, “Pemphigus Contagiosus (tropicus),” Brit. Med. Jour., April 29, 1899, P. 1021;
Finlay, “Pemphigus Contagiosus Tropicus,” Austral. Med. Gaz., 1898, p. 114; Brosin,
“Pemphigusübertragungen im Wirkungskreise einzelner Hebammen” (2 epidemics; in
a total of 64 confinements 18 cases, 7 of which died), Zeitschrift für Geburtshülfe und
Gynäkologie, 1899, vol. xl, p. 418; P. Richter, “Ueber Pemphigus neonatorum,” Derma-
tolog. Zeitschr., 1901, vol. viii, Nos. 5 and 6, reviews most thoroughly the whole subject
(over 100 pages, with 20 pages of references); he concludes that the dermatitis exfolia-
tiva neonatorum of Ritter is a variety, and that pemphigus neonatorum also bears a
relation to impetigo contagiosa, the characters of the newborn skin being responsible
for the clinical differences; it is due to the presence of a staphylococcus of a doubtful
nature, with a group, more malignant, infected with streptococci or mixed staphylo-
cocci and streptococci. G. J. Maguire, “Acute Contagious Pemphigus in the New-
born,” Brit. Jour. Derm., 1903, p. 427 (indicative of its identity or allied nature to
bullous impetigo contagipsa); Adamson, “Pemphigus Neonatorum in the Light of
Recent Research,” ibid., p. 447 (conclusion as to its being an infantile form of impetigo
contagiosa); Crary, “A Case of Acute Septic Pemphigus,” Jour. Cutan. Dis., 1906, p.
14 (with review and bibliography); Schwartz (Geo. T. Elliot‘s Service), “An Epidemic
of Pemphigus Neonatorum,” Bull, of Lying-in Hosp. of New York, June, 1908 (with
case and histologic illustration; there were 27 cases in all, 22 of the 27 developing be
tween the fourth and seventh day; 7 died and most of these died on the fourth to tenth
day of the disease; cultures from blebs, before and after death, showed only a staphy-
lococcus; there was distinct evidence of the contagious nature of the disease; the mild
cases, running a benign course, would have been looked upon, the writer states, as
impetigo contagiosa; Foerster, “Pemphigus Neonatorum, or Bullous Impetigo Con-
tagiosa of the New-born,” Jour: Amer. Med. Assoc, 1909, vol. liii, p. 358 (review, with
literature references).
376
INFLAMMATIONS
by others indicate, should be viewed as probably a type, possibly a
variant or contaminated type, of bullous impetigo contagiosa.1 Two
forms are usually distinguished, the grave type, which sometimes re
sembles pemphigus foliaceus and Ritter‘s disease, and a mild or benign
form. The mild type, of which a number of instances have been re
corded (01shausen and Mekus, Ravogli, Corlett, Kilham, Padosa,
Crocker, Knocker, and others), is usually entirely free from systemic

Fig. 90.—Acute pemphigus, with bleb walls largely rubbed off or collapsed;
simulated the lesions of an impetigo contagiosa in the earliest part; in some places
patches becoming larger by a spreading undermining serous exudation; lesions were
almost all more or less flaccid and flat; fatal ending.
disturbance, is of acute onset, and is seen in the newborn, usually in
the first several days of life. The lesions are, as a rule, not very numer
ous, and while they may be seated upon any part, are observed most
frequently or abundantly about the lower trunk and thighs. The
eruption may however, be quite extensive and of general distribution.
A favorable termination is reached in the course of a few weeks.
1 It is not improbable that even dermatitis exfoliativa neonatorum might be very
properly viewed in the same light.
PEMPHIGUS 377
On the other hand, cases are reported (Tilbury Fox, Staub, Peter,
Greer, Moldenhauer, Klemm, Brosin, and others) of severe and grave
characters. The eruption may be somewhat sparse or abundant, and
there is accompanying febrile action as observed in ordinary acute
pemphigus cases already described, with septic symptoms; or there
may be practically absence of fever, and yet the cases terminate fatally
(Brosin).
Pemphigus Chronicus.—Under chronic pemphigus belong most of
the cases usually met with, and to which the name of pemphigus vulgaris
is also applicable. It is, like other varieties, rare, and especially
in this country. Its chief distinction from the others is that the blebs
continue to appear incessantly, the skin being, as a rule, never free.
On the other hand, there may be shorter or longer intervals of compara
tive or complete freedom. The lesions appear irregularly, one or several
at a time, or there are distinct crop-like exacerbations, the blebs appear
ing in numbers. Probably most commonly they make their appearance
in numbers for several days or more; these subside, crust over, and dis
appear, during which time and for a few weeks or longer scattered lesions,
in scanty number, arise, and then another moderate or extensive out
break manifests itself, and so the malady continues indefinitely. The
mouth and throat in occasional cases are also noted to exhibit the erup
tion, and exceptionally the disease may have its beginning in these parts.
In rare instances the conjunctivæ (pemphigus conjunctivæ) are also
invaded, and sometimes accompanied by shrinking of the parts (von
Graefe, Morris and Roberts, Fuchs, and others) ,1 The blebs are usually
well distended, pea- to small egg-sized, scattered, or often close together,
several occasionally coalescing, although there is but little tendency
to grouping. A slight admixture of blood is sometimes noted, and
in exceptional cases this may be quite decided (pemphigus hæmorrhagi-
cus). An individual lesion, as in the other varieties, runs its course,
and crusts over in several days to two weeks. No permanent trace
is left by the eruption, but on areas frequently covered with recur
rent lesions slight pigmentation may show itself. In the mild cases
there are no constitutional symptoms; in others chilliness and febrile
action preceding or accompanying the original outbreak, subsiding
and again presenting at the time of the exacerbations; in still others
of the more extensive type the systemic disturbance is more or less
continuous. The subjective symptoms of burning, soreness, and
itching (pemphigus pruriginosus) may be present in variable degree;
itching is rarely troublesome and often absent. The disease may
finally end in recovery or terminate fatally, its course being usually
long and indeterminate.
1 Morris and Roberts, “Pemphigus of the Skin and Mucous Membrane of the
Mouth, Associated with ‘Essential Shrinking’ and Pemphigus of the Conjunctivæ,”
Brit. Jour. Derm., 1889, p. 176, and Monaishefte, 1889, vol. viii, p. 437 (a report of a
case, with colored plate, and a tabulation and references of 28 previously reported
cases); Meneau, Jour. mal. Cutan., Jan., 1905, gives an extensive review of different
forms of pemphigus as involving the mucous membrane, especially of the conjunctiva,
nose, mouth, throat, and larynx (with complete bibliography); Cocks, Jour. Amer.
Med. Assoc, Nov. 24, 1906, p. 1736, records a fatal case in which the eruption was
limited to the mucous membranes.
378
INFLAMMATIONS
Pemphigus Foliaceus.1—This variety, which is extremely rare, may
assume its peculiar features from the start or it may develop from an
acute or chronic pemphigus of the ordinary character; in other in
stances it has begun as a superficial generalized cutaneous edema
(Quinquard), as a scaly greasy surface (Besnier), as a dermatitis her-
petiformis (Hallopeau and Fournier). It is characterized by the
formation of blebs so rapidly and so quickly repeated that the dis
tended bulla is not seen. It is flat and but slightly raised, and is scarcely
dried to a crust before another flaccid lesion forms beneath. Or the
blebs appear, but instead of being distended and elevated, are flaccid
and flat, become purulent, break or are accidentally ruptured, and
then a gradual undermining of the surrounding epidermis is noted.
The eruption is usually abundant and generally distributed, and may,
1 Literature of pemphigus foliaceus: Nikolsky, “Contribution a la question du pem
phigus foliacé de Cazenave,” Thèse de doctorat, Kieff, 1896 (refers cases of Cazenave,
Plieninger, Bazin, Guibout, Meyer, Munro and Swarts, Sormani, Besnier (2 cases),
Hallopeau and Fournier (3 cases), Petrini (3 cases), Regensburger, and Dumesnil de
Rochemont—17 cases in all); Lausac, “Du pemphigus foliacé mixte primitif,” Thèse de
doctorat, Toulouse, 1898 (reports 1 case and refers to 28 cases previously observed by
others—brief abstract of his own case and conclusions in Annales, 1898, p. 1040;
Biddle, “Pemphigus foliaceous or Dermatitis herpetiformis,” Jour. Cutan. Dis., 1897,
p. 203; Sherwell (1 case, with photo), Arch. Derm., 1877, P. 97, and (same case—recov
ery and relapse), Jour. Cutan. Dis., 1889, p. 453; Graham (1 case), Canadian Jour.
Med. Sci., June, 1879; Hardaway (1 case), Jour. Cutan. Dis., 1890, p. 22; Munro and
Swarts’ case (ibid., 1891, pp. 332 and 423), already named in Nikolsky‘s paper, seems
to partake of the nature of both pemphigus foliaceus and pemphigus vegetans; Klotz
(1 case), Amer. Jour. Med. Sci., Dec, 1891; Nasarow (1 case), Dermatolog. Zeitschr.,
1899, vol. vi, p. 719; Nazaroff (1 case), Roussky Archive Patologgi, Feb., 1900—abstract
in Brit. Jour. Derm., 1900, p. 258; Hellier (1 case—infant (pemphigus neonatorum?),
Brit. Journ. Derm., 1899, p. 18; Savine (1 case), Jour, de med mil. russe, July, 1897;
abstract in Annales, 1898, p. 597; Hallopeau et Constensoux (1 case with associated
osteomalacia), Annales, 1898, p. 979; Lindstroem (3 cases), ibid., 1898, p. 1026; Leredde,
“Etude sur le pemphigus foliacé de Cazenave,” ibid., 1899, p. 601 (a study of path
ology and pathologic anatomy, with some literature references); Fabry, Archiv, June,
1904, p. 183 (1 case, beginning with redness and scaling, showing at first a suggestive re
semblance to pityriasis rosea and eczema marginatum developing into pemphigus
foliaceus); Brousse and Bruc, Annales, 1905, p. 853 (1 case; began with an erythematous
eruption, intense general itching, followed by bleb formation, which became generalized,
and in a month had developed into the exfoliative type; autopsy report and 1 clinical
and 1 histologic illustration); R. Cranston Low, Brit. Jour. Derm., 1909, pp. 101 and
135 (2 cases, both women; a third case, with symptoms of both dermatitis herpeti-
formis and pemphigus foliaceus; good review of the subject, discussion of a suggestive
occasional relationship with dermatitis herpetiformis and full bibliography; several
case illustrations); ibid., 1911, p. 1, a fourth case, woman aged fifty-two, of two years’
duration, at first diagnosed as dermatitis herpetiformis; out of 3 cases only 1 (the
last) gave a culture of the bacillus pyocyaneus; of the previous cases, case 1, the skin
condition still remains in statu quo; the case 3 has remained fairly well, but has
occasional recurrences of an eruption of the nature of dermatitis herpetiformis; Scha-
lek, Jour. Amer. Med. Assoc, July 2, 1910—male, aged thirty-six; C. J. White, Boston
Med. and Surg. Jour., May 4, 1911 (case report—female aged seventy-three, death nine
to ten months after original outbreak); Hazen, “Pemphigus Foliaceus,” Jour. Cutan.
Dis., 1910, p. 118; male, Hebrew aged thirty; had begun about year before coming
under observation; bacillus pyocyaneus was demonstrated in circulating blood, urine,
and non-purulent vesicles, and over the entire cutaneous surface; staphylococcus was
a secondary invader; and ibid., 1912, p. 325, second case in negro woman, aged fifty-
one, dying about five months after its first appearance; cultures from the blood, from
the skin at large, and from the outside of the vesicles, from old vesicles, and from
ruptured vesicles, gave the staphylococcus albus; cultures from fresh, unruptured
vesicles always gave bacillus pyocyaneus in pure culture; autopsy; cultures were
made from the heart’s blood, liver, spleen, and kidneys, and all gave a pure growth
of the bacillus pyocyaneus; histologic illustrations and bibliography.
PEMPHIGUS
379
indeed, involve almost the entire surface. In the latter instances a pic
ture is presented of extremely flaccid, scarcely elevated, seropurulent
or purulent variously sized blebs, with the fluid bulging them out at the
most dependent portion; ruptured lesions with a serous or seropurulent
undermining of the immediate surrounding epidermis; thin crusts with
rapidly forming exudation beneath, and large red, raw, oozing sur
faces where the crusts have been removed or rubbed off, and where
the exudation is so rapid that a new crust cannot form. Exception
ally the surface remains, temporarily at least, almost dry, the condi
tion resembling dermatitis exfoliativa. Fissuring occurs, especially
about the joints, and there is a pervading foul odor about the patient.
In extreme cases the nails and hair are brittle and sometimes shed,
the eyes are sore-looking, the conjunctivæ may become involved, the
mucous membranes share in the disease, and with increasing gravity
of the constitutional symptoms, and, in a majority of the cases, the
patient finally succumbs from exhaustion, pyemia, or from some inter-
current disease. Exceptionally there are long intervals of freedom
(Sherwell). The malady is rare, but there has been a gradual addition
to the number of reported cases since the disease was first described
(Cazenave, 1850); in this country cases have been recorded by Sherwell,
Graham, Hardaway, Klotz, Munro and Swarts, Hazen, C. J. White, and
a few others.
Pemphigus Vegetans.1—This variety, also called erythema bullosum
1 Literature of pemphigus vegetans: Crocker, “Pemphigus vegetans (Neumann),”
Brit. Med. Jour., March 16, 1889, and London Med.-Chirur. Soc‘y Trans., 1889, vol.
lxxii, p. 233 (a bibliography of cases to date is given); Mapother (1 case), ibid, (re
ferred to in the discussion); Müller, Monatshefte, 1890, vol. xi, p. 427 (2 cases, with
2 plates presenting 4 histologic cuts; a brief review of 22 other cases from literature,
with references, are given); Hyde (1 case), Jour. Cutan. Dis., 1891, vol. ix, pp. 412
and 459; Lowe, Lancet, May 23, 1891; Haslund, Hospitalstidende, 1891 (quoted by
Crocker); Herxheimer (3 cases, “Festschrift der Städtischen Krankenhauses in Frank
furt A. M.,” Archiv, 1896, vol. xxxvi, p. 141; Köbner (2 cases), Deutsches Archiv für klin.
Medicin, vol. liii, and vol. lvii, abstracts in Annales, 1894, p. 890, and 1897, p. 816;
Luithlen, “Pemphigus vulgaris et vegetans,” Archiv, 1897, vol. xl, p. 682; Tommasoli,
Archiv, 1898, vol. xliv, p. 325; Neumann, Wien. klin. Rundschau, 1900, No. 1, p. 1;
Pini, Giorn. ital., 1898, p. 354 (chemical experimental researches)—brief abstract in
Annales, 1899, p. 505; Phillipson, et Filed (1 case), Giorn. ital., 1896, p. 354; Ludwig
(1 case), Deutsch. med. Wochenschr., 1897, p. 267; Mracek (1 case), abstract in Annales,
1898, p. 919; Duhring (1 case), Cutaneous Medicine, part ii, p. 456; Zumbusch, “Ueber
Zwei Fälle von Pemphigus Vegetans mit Entwicklung von Tumoren,” Archiv, 1904,
vol. lxxiii, p. 121 (mild course with pedunculated papillomatous growths in 1 case;
large areas of papillomatous development in 1 case on forearms, leg, and soles of feet
(Dermatitis vegetans (?)); Jamieson and Welsh, Brit. Jour. Derm., 1902, p. 287, and
Dyce Duckworth, ibid., 1903, p. 26, and 1904, p. 245 (histologic report by Little, ibid.,
p. 138), each reports an extensive case—both fatal; Hamburger and Rubel, Johns Hop
kins Hosp. Bull., April, 1903, p. 63, report a fatal case, and review the literature; Zum-
busch, Archiv, 1905, vol. xliii (2 cases with development of tumors, 2 colored plates);
Ormsby and Bassoe (an acute fatal case with autopsy), Jour. Cutan. Dis., 1905, p. 294;
Ravogli, ibid., 1906, p. 311; Winfield, ibid., 1907, pp. 17 and 71 (with illustration), re
ports a fatal case with autopsy, and gives a brief analytic review of reported cases with
references; Constantin, Annales, 1907, p. 641 (case with features of dermatitis herpeti-
formis and pemphigus vegetans); W. Fox, Brit. Jour. Derm., 1908, p. 181 (case with
illustration of vegetations in axillae developing upon an ordinary pemphigus, vegetating
tendency subsequently disappearing, the malady assuming the type of a somewhat
mild pemphigus); MacCormac, ibid., p. 277 (vesicles appearing nine days after child
bed, first about the genitalia; later, vesicles and bullæ becoming more general, the
vegetating tendency about axillae and lower abdomen; death in three and one-half
months—references as to bactiorologic findings) Pernet, “Pemphigus Vegetans and
38o
INFLAMMATIONS
vegetans (Unna) is the rarest of all, and was first described (Neumann)
in 1886; since then other cases have been reported (Crocker, Hyde,
Haslund, Hutchinson, Riehl, Duhring, and others). The earliest
manifestations are usually to be seen in the mouth, throat, or lips, and
consist of whitish or reddish plaques; soon the ordinary blebs appear
on the integument, and these may at first maintain the character of
ordinary pemphigus, but after a while, instead of going through the
crusting and disappearance, as usually noted, vesicles or blebs form
around a crust; the base of such a patch becomes inflamed, often edem-
atous, covered with a viscid, offensive secretion, and finally exhibits
papillomatous or condyloma-like vegetations. Several such plaques
become confluent and form large areas. This peculiar development is
seen most commonly about warm and moist surfaces in close contact,
as about the genital, anal, and axillary regions. With increasing
constitutional symptoms which are usually present from the beginning,
the disease, with rare exceptions, finally ends fatally. In favorable
cases the process gradually declines; these seem to be chiefly those
in which the eruption was scanty and mainly about the mouth (Hutch-
inson). The malady is sometimes variable in its course, and occasionally
presents here and there distinct blebs in which the vegetating tendency
is not displayed. Exceptionally there is observed a combination of
its own peculiar manifestations with the symptoms of pemphigus
foliaceus. There is usually temperature elevation, somewhat variable,
it is true, determined by the extent and gravity of the disease; it is
usually more marked at periods of exacerbation of the cutaneous
phenomena. On the other hand, the body-heat is noted at times to be
below normal.
Etiology.—Pemphigus is, fortunately, extremely rare, and much
more so in this country than in Europe. It is met with in both sexes,
with probably a slight preponderance in females; it is more frequent
in infants and children than in adults. The causes are obscure. It is
not due to syphilis, although this latter does give rise to a pemphigoid
eruption, but one entirely different in its character, course, and behavior.
It is not hereditary; the cases of hereditary tendency to bullous develop
ment upon the slightest local irritation belong to epidermolysis bullosa
(q. v.). It is probable that the several so-called varieties are due to dif
ferent causes, or at the least the ingrafting of an accidental factor upon
the same disease process. Acute pemphigus sometimes has its origin
in a septic wound (Pernet and Bulloch, Hadley and Bulloch); from, in
infants, a disease of the navel and from puerperal processes in the mother
(Staub, Peter, Greer). Pernet and Bulloch's studies, as well as such
cases as that reported by Bowen, point strongly toward animals or their
the Bacillus Pyocyaneus,” Brit. Med. Jour., October 15, 1904 (1 case) and “A Case of
Pemphigus Vegetans, ibid., Sept. 24, 1910 (1 case); Pollitzer, “Pemphigus Vegetans”
(starting as a condylomatous patch at anus in male aged fifty-nine—death in about six
months), Festschrift zur Vierzigjährigen Stiftungsfeier der Deutschen Hospitals, New
York, 1911, p. 546; abstract in Brit. Jour. Derm., 1911, p. 335; Rutherford, Brit. Jour.
Derm., 1910, p. 118 (1 case—acute, death in seventeen weeks); Hartzell, “A Case of
Pemphigus Vegetans, with Special Reference to the Cellular Elements Found in the
Lesions,” Jour. Cutan. Dis., 1910, p. III. Bottelli, Giorn. ital., full abstract in Brit.
Jour. Derm., 1911, p. 371, began during pregnancy; bacteriology negative; death.
PEMPHIGUS 38l
products as a frequent source; this may, too, explain the cases following
vaccination occasionally, as, for instance, Howe's cases. Bowen calls
attention to the similarity of some cases of “foot and mouth disease”
in cattle to acute pemphigus in man. Doubtless, in many of these
acute cases just referred to, the actual underlying factor is a strepto-
coccic infection. The bacillus pyocyaneus has also been credited with
being the cause in some cases.1 Johnston2 believes we have evidence of
the existence of an autotoxic factor in the production of pemphigus and
other bullous diseases, a view which, it seems to me, has much in its
favor, but this autotoxic factor may be of varying nature and origin.
Other factors which seem to be of moment in the production of the dis
ease are chills (Schwimmer, Crocker), nervous influences, such as periph
eral nerve injuries (Mitchell, Morehouse and Keen, Mougeot, Leloir),
diseases of central nervous system (Charcot, Balmer, Leloir, Kopp,
Schwimmer, Brissaud, and others), degenerative changes in the periph
eral nerves and nerve-centers (Déjerine, Quinquaud, Jarisch, Mott and
Sangster, and others), functional nervous disturbance, and hysteria—
pemphigus hystericus3 (Kaposi, Hardy, Jarisch, Duhring, and others).
Against these evidences must, however, be quoted the observation
(Kaposi and Weiss) that in 9 fatal cases, in only 1 was there structural
nerve alteration—diffuse sclerosis of cord.
That the derangement, functional or organic, of the nervous system
is of etiologic importance is borne out by the cases reported by the
writers just referred to, and by the experience of almost all others
who have to do with this disease. Whether the action is a direct one
or merely contributory to a successful parasitic invasion or infection is
an unsolved question. At all events, whatever the rôle of the nervous
system may be in the chronic variety, there can scarcely be a doubt
that an important etiologic factor in many of the acute cases, and
especially those in infants and young children, particularly those of
epidemic and contagious character, is to be found in micro-organisms.
Such findings have been recorded by a number of observers (Alm-
quist, Escherich, Peter, Luithlen, Gibier, Demme, Sahli, Claessen,
Whipham, Holt, Beck,4 and others), but there has not been sufficient
1 Petges and Bichelonne, “Septicémie a bacille pyocanique et pemphigus bulleux
chronique vrai,” Annales, 1909, p. 417, report a case, review the subject, with refer
ences, and conclude that the bacillus pyocaneus can play a rôle both in chronic bullous
pemphigus and pemphigus vegetans; Hazen (loc. cit.) found this organism in two cases
of pemphigus foliaceus and believes it pathogenic in some cases.
2 Johnston, Brit. Med. Jour., Oct. 6, 1906.
3 C. J. White, “Recurrent, Progressive, Bullous Dermatitis in a Hysterical Subject,”
Jour. Cutan. Dis., 1903, p. 415, reports a curious case of bullous lesions, the outbreak
beginning usually on an extremity, and then extending upward, with periods of freedom,
and later involvement of other parts (4 other somewhat similar cases in literature are
briefly described, with references to these and other papers on allied subjects). Coffin,
Boston Med. and Surg. Jour., April 27, 1911, p. 612, gives details of a case—patient,
woman aged fifty-seven—in which oral cavity, epiglottis, and larynx were involved for
four years without accompanying cutaneous manifestations: two years after the onset
the eyes became involved; and two years later the skin became involved for the first
time, and one year before her death (five years after beginning), blebs appeared over
entire body; death from sepsis starting in a lesion on the foot.
4 Lipschütz, Archiv, 1912, cxi, No. 3, p. 675—abstract in Jour. Cutan. Dis., March,
1913, (elaborate study based on 11 cases of chronic pemphigus) has found two distinct
parasites in the serum contents of the bullæ; one he names the “cystoplasma oviforme,”
382 INFLAMMATIONS
uniformity to warrant positive conclusions, although the majority of
observers found, in pemphigus neonatorum,1 staphylococcus aureus
and albus; and some were able to produce the disease by inoculation
from lesions (Moldenhauer, Koch, Vidal), and also by inoculation from
cultures (Almquist, Strelitz). A diplococcus has been found by several
observers in acute pemphigus (Demme, Claessen, Bulloch, Whipham,
Beck). Investigations by others in both these directions have, how
ever, not met with the same positive results. The acute cases resulting
from septic infection already referred to point likewise to micro-organ
isms as a cause. The microbic view is also supported by the series of
cases of pemphigus neonatorum occurring in infants cared for by the
same widwife, an observation repeatedly made (Corlett, Knocker, and
several others). It is probable that most of these are examples of
bullous impetigo contagiosa, as instances of transference to older mem
bers of the family, etc., have occurred, and in whom the lesions are
essentially those of this latter disease, a view which is held by most
observers (Pontoppidan, Faber, Crocker, Duhring, and many others).
Another view of the etiology of pemphigus formerly held was that
the malady is due to defective kidney elimination, and occasional acute
cases are noted to follow or be associated with organic kidney disease.
Urine examinations in most instances, however, disclose nothing. As
in other bullous diseases, eosinophilia has been noted (Leredde), and a
diminution of the red blood-corpuscles observed (Hallopeau and Leredde,
Nikolski).
Pemphigus, especially the acute form, has also been observed to
follow rheumatic fever, the exanthemata, diphtheria, and other acute
systemic disorders.
Pemphigus vegetans2 seems, as noted by Hutchinson, Danlos, Brocq,
and others, much more common with those who live in the country—
2 cases that came under my observation were from country districts.
Pathology.—In connection with pemphigus lesions on the skin
organic changes have been noted, as already remarked, in other struc
tures, more especially the nervous system in its various parts, centrally
to peripherally,3 the liver and kidneys have also exhibited disease in
measuring 1.5 to 2.7 micra, with an eccentric nucleus, extending through the margin
or just bordering the periphery; in the same case it may be absent at times and times
when present in great numbers; the other organism, he names “anaplasma liberum,”
is considerably smaller, has practically no cytoplasm, being entirely made up of
chromatin or nuclear substance. The exact relationship of the two is not clear. He
found the same present in cases which pass as dermatitis herpetiformis.
1 Both Whitfield (Brit. Jour. Derm., 1903, p. 221) and Macleod (Brit. Med. Jour.,
1903, p. 1278) obtained pure cultures of a streptococcus.
2 Stanziale, Annales, 1904, p. 15, found in a case of pemphigus vegetans a diplo-
bacillus (probably identical with the small diplococcus of Waelsch), and a pseudo-
diphtheritic bacillus. The latter, he thought, played a rôle in the production of the
vegetating lesions. Hamburger and Rubel, loc. cit., also isolated: a pseudodiphtheritic
bacillus.
3 Jamieson and Welsh, loc. cit., found in a well-marked case of pemphigus vegetans
distinct degenerative changes of a special character in the nerve-cells of the spinal cord,
and to a less pronounced extent of the sympathetic ganglia, and the cerebral cortex; con
sisting “of an evidently slowly progressive rarefaction of the chromophile bodies of the
protoplasm, more especially in the perinuclear zone, formation of minute vacuoles in
the altered portion of the protoplasm, swelling of the cell-body, disintegration of the
nucleus, and, finally, destruction of the whole element.”
PEMPHIGUS
383
some cases. To a great extent, or at least in many instances, the
cutaneous manifestations must be considered but a part of a systemic
process or infection. This belief is supported by the findings of micro-
organisms referred to in etiology.
Pathologic anatomy1 discloses (Robinson, Crocker, Luithlen, Unna,
Gilchrist, Jarisch, and others) that the local changes in the cutaneous
lesions are slightly varied, dependent, doubtless, upon the degree of
inflammatory action and the stage of formation, although the bleb is
more superficial than obtains in herpes. The roof-wall is the upper
horny layer, and the base the rete; but in some instances the inside of
the roof shows a layer of rete cells, and in others the corium is the floor
of the lesion. The bleb is doubtless due to a sudden effusion from the
vessels of the corium, probably following paralysis and dilatation of the
vessels.2 In the early stage of its formation, in most lesions, inflamma
tory signs are slight; in others they are present, usually but to a moderate
degree. The papillae are edematous; dilatation of the vessels, emigration
of polynuclear leukocytes, and a variable amount of serous infiltration
of the tissues are noted. In pemphigus vegetans are found (Neumann,
Riehl, Kaposi, Unna3) marked hypertrophy of the papillae and pro
nounced proliferation of the rete, with outgrowth of the same; enlarge
ment of the superficial blood-vessels and edema of the upper layers of
the corium.
The contents of the lesions are neutral or alkaline in reaction and
composed of serum, to which are added later pus-cells, epithelial cells,
and fat; ammonia has been found in it, as well as in the urine; phos
phorus has also been found and thought to be due to nerve dis
integration. An increase of eosinophile cells has, as already stated,
in some instances been noted both in the bullæ and in the blood,
but as yet no significance can be assigned to this increase, as it is
observed in vesicles and bullæ of other maladies and even in those of
artificial origin.4
1 Jarisch, “Zur Anatomie und Pathogenese der Pemphigusblasen," Archiv, 1898,
vol. xliii, p. 341; Robinson, section, drawing, and description in Duhring's Cutaneous
Medicine, part ii; Gilchrist, ibid.; Kromayer, Dermatologische Zeitschrift, 1897, vol.
iv; Kreibich, Archiv, 1899, vol. 1, pp. 299, 375; Luithlen (Pemphigus vulg. et veg.),
Archiv, 1897, vol. xl, p. 682, and (Pemphigus neonatorum), Wien. klin. Wochenschr.,
1899, p. 69.
2 According to Weidenfeld‘s investigations (“Beiträge zur Klinik und Pathogenese
des Pemphigus,” Vienna, 1904, a monograph based on 18 cases: 9 pemphigus vulgaris,
4 pemphigus serpiginosus, 5 pemphigus foliaceus, and 1 pemphigus vegetans), he found
that in some cases of pemphigus, pressure would always provoke a bleb, in other cases
pressure had absolutely no influence, while in a third group it was variable—sometimes
pressure producing a bleb and sometimes not. In the stages of improvement none could
be provoked, but as soon as the general condition (eruption, etc) showed increase and
aggravation, blebs could again be provoked by pressure. The author explains this upon
the assumption of a variation or disappearance and reappearance of some noxious mate
rial having a damaging influence on the circulatory system.
3 Hartzell (loc. at.) found in a flaccid bleb from a case of pemphigus vegetans in
addition to eosinophiles, “a moderate number of large round cells quite uniform in size
and appearance, lying here and there among the other cells, stained with eosin, con
taining a large cavity with a limiting membrane more deeply stained than the ring-
like body of the cell.” They resembled the “ballooned” epithelium found in zoster,
etc, although the writer inclined to believe them quite distinct.
4 Hartzell found the eosinophiles extremely numerous in a bleb of pemphigus vege-
tans and scanty in number in a bleb from pemphigus vulgaris.
384
INFLAMMATIONS
Diagnosis.—The disease is to be distinguished from erythema
bullosum, urticaria bullosa, impetigo contagiosa, dermatitis herpeti-
formis, and the bullous syphiloderm.
In erythema bullosum the blebs are a part of an eruption (ery
thema multiforme) in which other characteristic features are usually
present; even when all the lesions are bullous there is likely to be a
circinate or ring-like configuration with some, and the eruption is gen
erally limited to, or more abundant on, certain regions, as the hands
and forearms—erythema bullosum never has a general distribution.
Moreover, the blebs frequently spring from erythematous or inflam
matory skin, and the disease runs a rapid course without, as a rule,
any persistent or marked systemic symptoms.
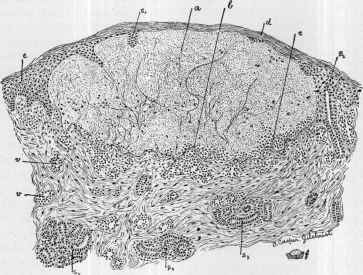
Fig. 91.—Pemphigus—a beginning bleb (a) between corium and the epidermis,
the bared papillæ (b) forming the base; acute inflammatory changes in the papillary
layer of the corium, with marked serous exudation, particularly about the vessels;
reticular part of the corium and the sweat-glands (s3, s4, s5) are practically normal,
except where the sweat-ducts (s1, s2) are involved in the bleb-formation: d, corneous
layer; e, rete; v, v, blood-vessels; c, cell masses at base;f, about the natural size of bleb
examined (courtesy of Dr. T. Caspar Gilchrist),
The bullous syphiloderm is usually observed in infants in the first
few days or weeks of life; and the lesions are often seen on the palms
and soles, parts not commonly involved in pemphigus. Moreover,
the syphilitic blebs soon become puriform, form thick crusts, and
under which, as a rule, ulceration is noted. In syphilis of this type
other characteristic symptoms are always to be found. Pemphigus
vegetans bears strong resemblance to the vegetating syphiloderm; in
this latter, however, the disease remains more or less limited to the
genital region and around the anus, with but little disposition to spread
extensively, as is observed in pemphigus. Moreover, in syphilis a
positive destructive tendency is sometimes noted, and there is absence
PEMPHIGUS
385
of any tendency to bleb-formation, usually seen at some stage of pem
phigus vegetans. The clinical history, the presence or absence of other
syphilitic lesions or symptoms, examination for spirochætæ, and the
Wassermann test must sometimes be utilized. In pemphigus, too,
slight or severe constitutional involvement is usually noted. Pem
phigus foliaceus and dermatitis exfoliativa are sometimes confounded,
but the dry character in the latter and the absence of mouth involve
ment and any tendency to bleb-formation are different from what are
observed in pemphigus.
Eczema rubrum and pemphigus foliaceus have, in a general way,
some resemblance, but the former is never universal, and, indeed,
rarely extensive; the crusting of the former is usually less pronounced,
the crusts being in small flakes, whereas in pemphigus they are often
of considerable size; moreover, blebs are not seen in eczema, and the char
acters of the general symptoms observed in pemphigus are wanting.
It is scarcely possible to confound the blebs occasionally noted in
scabies with pemphigus; in the former there is never present more than
a scant number, and the other eruptive lesions, together with the dis
tribution and history, are entirely different from the picture of pemphi
gus. The differentiation from bullous urticaria, impetigo contagiosa,
and dermatitis herpetiformis will be found discussed under those diseases.
Prognosis.—Too much caution cannot be exercised in express
ing a positive opinion as to the final outcome. As to acute pemphi
gus, the character of the outbreak, whether attended by active con
stitutional symptoms, the behavior of the lesions (whether serous,
purulent, hemorrhagic, or gangrenous), the extent of the eruption,
the previous and present health of the patient—all have a bearing.
Those cases in which more or less grave systemic disturbance presents,
and those, usually the same class, in which the lesions become rapidly
purulent or are hemorrhagic or gangrenous, are almost always fatal.
Involvement of the mucous surfaces is of unfavorable significance.1
Even slight systemic disturbance, especially chills, has a serious import.
The vegetating and foliaceous varieties rarely recover, but they may be
of months’ or years’ duration. The septic types, arising from a wound,
are grave. Almost all cases unattended by temperature elevation or
other constitutional symptoms get well, although the possibility of chang
ing to a severe type is to be kept in mind. In short, the prognosis for
the milder cases is usually favorable; for the extensive and grave erup
tions, serious. The prospect in children is much better than in adults.
In chronic cases the same features bear upon the ultimate prog
nosis: persistence and chronicity are the rule, and relapses are not un
common. Death usually takes place from general septic infection;
from gradual marasmus, sometimes with diarrhea; and occasionally
from sudden collapse.2
Treatment.—The treatment includes both constitutional and
1 According to Weidenfeld, “Beiträge zur Klinik und Pathogenese des Pemphigus,”
Vienna, 1904, those cases of pemphigus in which the malady begins in the mouth are
the gravest.
2 Klotz, Jour. Cutan. Dis., 1909, p. 242, reports such a case.
25
386
INFLAMMATIONS
local remedies. The systemic treatment, which is of essential impor
tance in the grave acute and in the chronic varieties, is, upon the whole,
to be based upon general principles, any possible etiologic factor being
corrected, modified, or removed, the general health built up, and the
digestive tract looked after. In fact, a careful study of the whole
economy should be made. The patient should have the benefit of good
hygienic conditions. There are, however, certain remedies which have
acquired deservedly more or less reputation of exerting a specific influ
ence. First in importance is arsenic (Hutchinson, Morris, and others),
given in safe but increasing doses up to the point of tolerance. The
drug has in some cases a controlling influence, and it is sometimes cura
tive; its use should be persisted in, as it is usually after long administra
tion that its beneficial effects are to be expected; it should also be con
tinued in small doses for some time after the disease has disappeared.1
Sodium cacodylate by hypodermic injection is sometimes valuable.
Strychnin and large doses of quinin are likewise useful in some instances.
These three remedies, arsenic, quinin, and strychnin, probably the most
valuable in this malady, can advantageously be prescribed conjointly.
Iron in full doses, cod-liver oil, and linseed meal (Sherwell) are also of
service in some cases. Opium, especially in the vegetating form (Hutch-
inson), pilocarpin, and atropin (Crocker), have exceptionally proved of
advantage. It is a good field for the trial of vaccines. Change of
scene and climate is of distinct value in some instances. The dietary
should be generous, but of a plain and substantial character.
Externally applications of a soothing nature are the most grateful.
It is a good rule to open and evacuate the blebs as soon as they form,
immediately applying one of the local remedies. The various lotions
employed in the acute type of eczema, especially those containing sedi
ments, are valuable, and should be applied freely by dabbing on or by
compresses; or, instead of lotions, the several dusting-powders named,
particularly those containing boric acid. In painful and extensive cases
linimentum calcis is grateful. Engman and C. J. White2 commend
the free and very liberal use of drying powder, the former using corn-
starch powder and the latter borated talc; the patient is actually to live
in the powder. Sometimes ointments, such as the zinc oxid ointment,
an ointment containing 1 dram (4.) of calamin to the ounce (32.), a mild
salicylic acid ointment, from 10 to 20 grains (0.65-1.3) to the ounce (32.),
and salicylated paste are comforting. In cases in which the disease is
more or less general, bran baths, starch baths, gelatin baths, and occa
sionally an alkaline bath, followed by the application of an ointment,
will prove acceptable. In the most severe types the continuous bath
1 Pollitzer, Festschrift des Deutschen Hospitals, 1911, p. 546, reports an apparent
cure of a case of chronic pemphigus with severe involvement of the mucous membranes
with large doses of arsenic; Sutton, Boston Med. and Surg. Jour., March 9, 1911,
reports a rapidly favorable result in a single case from a dose of salvarsan. In a case
at Philadelphia Hospital, with slight tendency to vegetating type, first under Dr.
Hartzell‘s care and subsequently mine, rapid temporary improvement was noted from
a dose of salvarsan, but later to another dose there was no response, the patient sub
sequently dying from the disease.
2 C. J. White, “The Dry Treatment of Certain Dermatoses,” Jour. Cutan. Dis.,
Dec, 1912, p. 705.
DERMATITIS VEGETANS
387
(Hebra) is to be employed. In cases in which itching is a more or less
prominent symptom carbolic acid may be added to the lotions or oint
ments employed; or the other applications employed to relieve itching,
as mentioned in the treatment of eczema, may be resorted to. In pem
phigus occurring in infants and young persons the same general plan
of treatment is to be followed.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |