| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
PELLAGRA
173
PELLAGRA1
Synonyms.—Lombardian leprosy; Erythema endemicum; Fr., Pellagre; Mal de
misère; L‘érythème pellagreux; Ital., Mal Rosso; Risipola Lombarda; Mal del Sole;
Scorbuto alpino.
Definition.—Pellagra is an endemic systemic disease, character
ized by cutaneous manifestations of an erythematosquamous and pig
mentary character, and associated with disturbances of the cerebro-
spinal system and the digestive tract. It is of endemic occurrence
in certain regions of Italy (Lombardy, Venetia, Æmilia) and Spain;
also in the Tyrol, Bukovina, and Roumania. Its first occurrence in
Spain is referred to the year 1735. In recent years sporadic cases
1 Some important literature of pellagra. Foreign: Tuke, Klinische und Ana-
tomische Studien uber die Pellagra, Berlin, 1893; Lombroso, Die Lehre von der Pellagra,
Berlin, 1898 (an exhaustive monograph with histologic cuts); Sandwith, “Pellagra in
Egypt,” Brit. Jour. Derm., 1898, p. 395; Raymond, “Les altérations cutanées de la
pellagre,” Annales, 1889, p. 627; Nicolas and Jambon, “Contributions a Petude de la
pellagre et du syndrome pellagreux Annales,” 1908, pp. 385 and 480 (review with full
bibliography); Sambon, Brit. Med. Jour., 1905, ii, p. 1272 (geographic and etiologic);
Manson, “Tropical Diseases”; Lavinder and Babcock‘s Translation of Marie‘s French
Monograph.
American: Searcy, “An Epidemic of Acute Pellagra,” Jour. Amer. Med. Assoc,
1907, vol. xlix, p. 37, and “Pellagra in the Southern States,” New Orleans Med. Jour.,
Oct., 1908, p. 413; Wood, “The Appearance of Pellagra in the United States,” Jour.
Amer. Med. Assoc, 1908, vol. liii, p. 274 (illustrated; a good review of the subject);
Babcock, “What are Pellagra and Pellagrous Insanity? Does Such a Disease Exist in
North Carolina, and What are Its Causes?” Report of Board of Health, South Carolina,
1907; Jour. South Carolina Med. Assoc, Nov., 1908; Amer. Jour. Insanity, April, 1908
vol. lxiv; Lavinder, “Pellagra: A Précis,” Public Health and Marine Hospital Service,
Washington, D. C, 1908; “The Prevalence of Pellagra in the United States,” ibid.,
1909; “Notes on the Prognosis and Treatment of Pellagra,” ibid., “Prophylaxis of
Pellagra,” ibid., and “Etiology of Pellagra,” New York Med. Jour., July 10, 1909; Wat
son, “Etiology of Pellagra. The Italian Maize Theory or the Theory of Lombroso,”
Jour. South Carolina Med. Assoc, Nov., 1908; and “Pellagra: Observations on the Dis
ease as a Result of Study of One Hundred Cases in South Carolina and Italy,” New
York Med. Jour., May 18, 1909, p. 936 (good review of the subject); Egan, “Pellagra
in Illinois: History, Etiology, and Symptomatology,” Bull. Illinois State Board of
Healthy Pellagra number, Aug., 1909 (review and references, and a number of illus
trations); “Transactions of Conference on Pellagra,” held in Columbia, S. C, Nov.
3-4, 1909, Jour. Amer. Med. Assoc, 1909, vol. liii, p. 1659; Hyde, “Pellagra and
Some of the Problems,” Amer. Jour. Med. Sci., Jan., 1910 (2 colored illustrations,
review and bibliography); Dyer, New York Med. Jour., 1909, p. 997 (cutaneous symp
toms); Howard Fox, New York Med. Record, Feb. 5, 1910 (cutaneous symptoms);
Siler and Nichols, “Observations on Pellagra at the Peoria State Hospital, Ill.,” New
York Med. Record, Jan. 15, 1910 (a study and an exposition of the disease in all its
phases; 175 cases among 2150 inmates in 1009; examinations of fecal matter disclosed
in 84.8 per cent, of the cases protozoal infection [amebæ, flagellate, and encysted forms]);
Reed, New York Med. Record, Jan. 22, 1910 (etiologic; calls attention to the fact that
the fungus diplodia has lately become sufficiently prevalent in America to attract the
attention of those engaged in growing maize, and its prevalence almost simultaneous
with the appearance of pellagra); King, “The Etiologic Controversy Regarding Pel
lagra,” Jour. Amer. Med. Assoc, March 12, 1910, p. 859 (gives a good review of the
conflicting opinions with references); Sambon, “Nature,” Oct. 17, 1910—abstract in
Jour. Amer. Med. Assoc, July 23,1910, p. 361—believes from his investigations that the
maize is not the cause, but that evidence points to its transmission to the individual by
an infected sand-fly; Albright, “Pellagra in Tennessee,” Southern Med. Jour., March,
1912, p. 69, states (Special Commission Report) that investigations in 64 out of 96
counties disclosed 316 cases; Knight, Jour. Amer. Med. Assoc, June 22, 1912, p. 1940,
reports 10 cases in one family—whole family—parents and eight children; specimen of
cornmeal examined and found to be unfit for human consumption. See also recent
book publications by Lavinder and Babcock, Niles, Roberts, and Edward Jenner
Wood.
174 INFLAMMATIONS
and small epidemics have been observed in other parts of the world;
and its appearance and development in the United States, more espe
cially in the Southern part, have been recently brought to notice by
Merrill, Searcy, Babcock, Zeller, Bellamy, Moore, Lavinder, Egan,
Siler, Wood, Watson, Thayer, and others.
Symptoms.—There are two types of the disease: the acute (ty
phoid type of Lombroso) and the chronic This latter is the common
one, and that which is usually described by the Italian writers.1 In the
recrudescences in the chronic cases the type may change to that of acute.
The disease usually appears in the spring, is frequently preceded
for several weeks or longer by lassitude, great fatigue, vertigo, headache,
anorexia, pain in the epigastrium, and diarrhea; sometimes associated
with sensations of weakness, especially in the lower extremities, and not
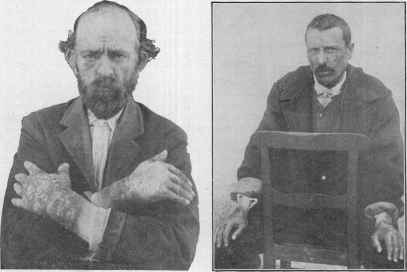
Fig. 31.—Pellagra: Showing involve Fig. 32.—Pellagra: Showing eruption
ment, with pigmentation, of hands, lower and pigmentation on hands and face (one
forearms, and, to a slighter extent, the face of Lombroso‘s cases; courtesy of Dr. J. J.
(courtesy of Dr. J. J. Watson). Watson).
infrequently with a feeling of dryness and burning in the mouth, and heat
in the stomach. Later in the course of the disease there may be an
associated stomatitis, with more or less salivation.
The cutaneous phenomena are, as a rule, the last to appear, and
these can be divided roughly into three stages: the first, congestion
or erythema; the second, with added scaliness, thickening, and pigmen
tation; and the third, a tendency to atrophic thinning. When first
presenting, therefore, the eruption is erythematous in character and
primarily dark red in color, which later becomes dark brown; and is
fairly symmetrical. It appears on uncovered portions, those which
1 Most Italian writers allege that the acute type is never primary, but is always a
profound exacerbation of the chronic form. Wood and others state, on the contrary,
from their study of the cases in our Southern States that at least 50 per cent, are of the
acute form.
PELLAGRA 175
are commonly exposed to the sun, as the back of the hand and lower
part of the forearms, face; and in persons who go barefooted, on the
lower part of the legs and dorsal surface of the feet. Raymond and
others have, however, observed it on the feet of those who are foot-clad,
and Wood and others have noted it on the sternum and the labia pudendi.
The skin, which assumes a reddish color, soon develops a variable degree
of thickening, and to these changes are added burning and itchy sensa
tions, and, later on, there may be loss of sensibility. The inflammation
may have its seat in the superficial or deeper layers. The epidermis,
especially the horny layer, seems to shrivel up, more conspicuously at
the border, and slowly desquamates, the amount of scaliness varying
somewhat in different cases and in different attacks; the underlying
surface appears red, and not infrequently is fissured. Occasionally the
gross appearances are those of a superficial burn in its middle and disap
pearing stages. Vesicles, bullæ, and petechiæ are also not uncommon

Pig 33—Pellagra: Showing the constant involvement, with pigmentation, of hands
and wrists (courtesy of Dr. J. A. Egan).
associated manifestations. Pigmentation takes place during and after
the attacks, the parts remaining more or less thickened. These latter
features become more pronounced with succeeding attacks. At the ad
vent of winter the cutaneous phenomena show signs of improvement, and
the disease gradually abates and, exceptionally, may disappear. Usu
ally, however, as late spring approaches, it recurs, and the disease may
thus repeat itself for several or more years, and, in addition to the
cutaneous changes, brings in its course muscular weakness and mental
despondency. These apparently free intervals are, as a rule, mere remis
sions in the malady, and not a disappearance with subsequent recurrence.
After repeated attacks the skin becomes wrinkled, thinned, lax, and takes
on a senile appearance, and presents a bluish-red or dark-brown color, and
tends to exfoliate in large flakes. The fingers become more or less fixed
in a semiflexed position. Gradually the patient becomes debilitated and
greatly emaciated, owing to digestive weakness and to frequent coexistent
diarrhea, and also, doubtless, as a result of the changes brought about
176
INFLAMMATIONS
by the involvement of the cerebrospinal system. Later, as the pulse
becomes weak and the muscular weakness increases, pains in the head
and spinal cord and convulsions present, stupor and melancholia develop,
and quite frequently insanity results; sooner or later a fatal termination
ensues. These last-mentioned symptoms may exceptionally be among
the earliest manifestations.
In the acute form of the malady the onset is more rapid and more
violent, with the typhoid symptoms usually pronounced. The toxemic
characters are predominant, while the skin and other phenomena may
or may not be more or less striking; exceptionally, the patient succumb
ing before the cutaneous changes are fully developed. While pellagra
is often considered an afebrile disease, during the active period there is
often a rise in temperature, usually slight.
Etiology and Pathology.—The disease develops at almost all
ages, but most frequently in those of mature adult age. In Italy it seems
confined to the poor and peasant class, but in our Southern States, while
more prevalent with these classes, the upper classes are also affected.
It is not contagious, nor is it now believed to be hereditary. It is met
with in almost all the European countries, being, however, peculiarly
frequent in Italy and Roumania. In our country it was scarcely known
until a few years ago, when its appearance in our Southern States, and
especially in institutions for the insane, in considerable numbers, was,
as already stated, noted. It has been attributed to the eating of damaged
maize. According to Neusser, the poisonous principle is developed in
diseased or fermented maize under the influence of the bacteridium
maidis. Paltauf and Heider, Macjocchi, Babes, Tizzoni and Panichi,
Wood, and others have also found various organisms, some similar, but
most of them different, to which they incline to attribute the disease.
Lombroso's investigations1 seem to attribute it to the causative action
of fermented maize toxins, and he claimed to have experimentally pro
duced symptoms apparently similar. On the other hand, Kaposi,
Scheiber, Manson, and others have observed the malady in those who
have never used this food, and Hardy also stated that he had had cases
in the Hospital Saint-Louis in which maize had played no rôle. These
and other observers have also called attention to the fact that there are
regions where maize is extensively cultivated and much eaten in which
pellagra is absolutely unknown. Alcoholic excess, poverty, poor hy
gienic surroundings, and exposure to the sun are predisposing factors, the
last considered by many as being almost essential, but some exceptions
to this are now known. It is not impossible that the peculiar distribu
tion of the eruption could also be ascribed to the circulatory weakness
and nerve influence.2 Blood investigations show a secondary anemia,
1 Lombroso's theory is that certain fungi and aspergilli form on maize if it is exposed
to moisture, these producing a toxin, which taken up into the system, causes pellagra.
2 Neusser has recorded that in Roumania the gypsy children who run about entirely
naked show the usual distribution of the eruption. In some of the American cases it is
not uncommon for covered parts to be coinvolved; more especially parts of the body
which are subject to pressure (Watson). Some of the Illinois suspected patients were
made to wear fenestrated gloves, the developing eruption being largely limited to the
exposed areas; on the other hand, patients not exposed to the sun, and bedridden patients
developed the eruption on the characteristic situations (Ormsby).
PELLAGRA
177
rarely a marked leucocytosis; blood is uniformly sterile and not infective
for ordinary laboratory animals (Lavinder).
The postmortem findings are pachymeningitis, sclerosis of the
brain and cord, and anemic and atrophic conditions of internal organs,
fatty degeneration, and pigmentary changes.1 The cutaneous changes,
according to Raymond, are essentially those of a mild congestion and
irritation, and more especially a hyperkeratinization with atrophy of
the rete.
One may, I believe, be justified in saying that as yet the aggregate
observations and experimental investigations are still lacking in con-
clusiveness as to the true and essential cause of the disease. It seems
not unlikely, from its ensemble of symptoms and its analogy to other
protozöal infections, that its cause may be found in protozoal organ
isms, a view suggested several years ago by Sambon, later by Terni,
and recently by several American observers, especially Siler and Nichols.2
Diagnosis.—Outside of the usual districts for the disease, some
difficulty might well arise in the diagnosis in the earlier period. The
most prominent characteristic signs are the parts affected (backs of
hands, lower forearms, face, and often dorsal surface of feet) and the
character of the eruptive phenomena—dermatitis, usually of a mild
grade, often simulating the appearance of a burn—with, especially
later, thickening and pigmentation; the frequently observed shriveling
of the horny layer, and occasionally almost the entire epidermis (usually
more marked at the borders), just before desquamating is to be con
sidered more or less suggestive.3 These symptoms and the associated
and sometimes precursory general disturbances of digestion, frequent
diarrhea, nervous involvement, melancholy, and other evidences of
mental despondency, will usually prevent error. If to these, say many
observers, is added the knowledge that the patient has lived largely on
maize, the diagnosis becomes more certain. It should not be confused
with another rare condition—pseudopellagra—observed in alcoholics
with peripheral neuritis.
Prognosis and Treatment.—In regions where the disease has
1 Spiller (Anderson and Spiller, Amer. Jour. Med. Sci., Jan., 1911) in a pathologic
report on material from 2 cases, and from a pathologic review of the subject (with
references) found “that the degeneration is caused by some toxic or infectious sub
stance affecting all parts of the cerebrospinal axis, producing cellular degeneration and
diffuse degeneration of nerve-fibers in the posterior and anterolateral columns; the
cortical degeneration of the brain is responsible for the mental symptoms”; Corlett
and Schultz (Jour. Cutan. Dis., 1911, p. 193) noted first changes in the nervous system,
structural changes in the nerve-cells and fibers leading to loss of ganglion cells and the
disappearance of the axis cylinder in the peripheral nerves supplying affected skin areas
and in those of the gastric mucosa; The Illinois Pellagra Commission (Dr. Ormsby,
Sec‘y) found the postmortem findings to be those of a generalized intoxication.
2Ormsby (Report of Illinois Pellagra Commission, Jour. Cutan. Dis., 1912, p.
589) states the Commission concluded that the disease appears to be due to infection
with some living organism; Sambon and Chambers’ (review of preliminary report
on the work done by Sambon and Chambers, in Egypt, Italy, Spain, Austria, Rou-
mania, France, and Hungary, on question of etiology, editorial in Jour. Trop. Med.
and Hyg., Sept. 2, 1912, p. 262) investigations seem to exclude the maize theory, direct
contagion, house infection, and hereditary transmission, and to point conclusively to
the insect-carried infection of pellagra.
3 Menage, Southern Med. Journal., March, 1912, p. 88, looks upon this shriveling
appearance as almost pathognomonic.
12
178
INFLAMMATIONS
long been endemic, the outlook, in slight attacks, is favorable, pro
vided the proper food can be given and the surroundings improved.
Severe cases are prone to prove fatal; the average duration is five years,
although it may continue for ten or fifteen. In communities where
the disease is new, as, for example, our Southern States, the prognosis
is grave, the majority of cases proving fatal, and the acute type prob
ably invariably so; the average duration is also less.
There are no specific remedies, the essential management consist
ing in placing the patient in good hygienic surroundings, and improv
ing the general health by good nourishing food and such tonics as may
seem indicated. Arsenic and iron preparations, especially the former,
and usually in the form of Fowler‘s solution, are the remedies upon which
most support has been placed, and which sometimes influence the disease
favorably; atoxyl has been lauded by a few, but Babcock, Lavinder,
Thayer, Wood, and others could not corroborate its alleged promptly
favorable action. Salvarsan has also been credited with some recoveries.1
In one recorded instance (Thayer) thyroid proved of promising value;
and in several instances (Cole and Winthrop) transfusion of blood cured
the patient. According to Siler and Nichols (Peoria State Hospital
observations) “mild cases recovered without therapeutic aid; severe
cases were not much benefited by Fowler‘s solution, atoxyl, or thyroid
tablets.”
Acrodynia.—Synonyms.—Erythema epidemicum; Cheiropodalgia; Fr., Acrodynie;
Mal des pieds et des mains; Maladie de Paris; Ger., Acrodynie.
This title was given by Chardon to a disease first observed in Paris
and in other parts of France from 1828 to 1830, occurring as an acute
epidemic and having some resemblance to both ergotism and pellagra.
Occasional cases are observed from time to time among soldiers and
prisoners, and exceptionally in others.2 Most cases have occurred in
Eastern countries. The malady is ushered in with constitutional symp
toms consisting of anorexia, nausea, vomiting, and diarrhea; and the
face, hands, and feet are noted to be swollen, and the conjunctivæ in
jected. It is accompanied by disorders of the nervous system, char
acterized by pricking and burning sensations; at first there is marked
hyperesthesia of the extremities, which in turn is followed by anesthesia;
severe pains in the extremities are one of the characteristic features of
the disease. Early in the course of the malady the eruptive phenomena,
make their appearance, and present as erythematous spots primarily on
the hands and feet, especially on the palms and soles, and spreading up
ward on the arms and legs, and sometimes involving the trunk. The
affected portions of the skin desquamate and are thickened and brownish ;
black pigmentation may supervene. The disease is afebrile and usually
runs its course in a fortnight to four weeks. In aggravated cases paresis,
edema of the limbs, and toxic spasms may ensue.
1 Nice, McLester and Torrance, “Pellagra Treated with Salvarsan,” Jour. Amer.
Med. Assoc, 1911, No. 12, lvi (successful in 3 cases).
2 Tholozan, “De l‘acrodynie,” Gaz. Méd. de Paris, 1861, pp. 647, 661, 689, 724,
and 821, has reported 20 cases and described the malady fully.
URTICARIA
179
The nature of the disease is obscure. Some observers attribute it
to a toxic agent affecting the nerve-centers, developed in damaged grain;
others recognize its analogy to pellagra and ergotism, and Marquez1
remarks upon the similarity of the general and local symptoms to those
resulting from chronic arsenical poisoning. In several of the fatal cases
inflammation of the spinal arachnoid has been noted.
The malady usually, however, except in those greatly debilitated
or in advanced years, runs a favorable course, recovery ensuing within
one or two months. Treatment is upon general principles. Counter-
irritation over the spine has been employed, and is generally advised.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |