| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
LICHEN PLANUS
213
LICHEN PLANUS
Synonyms.—Lichen ruber planus; Lichen psoriasis.
Definition.—An inflammatory disease characterized by pin-head
to small pea-sized flattened, glistening, crimson or violaceous papules,
with often a slight central depression, and often an irregular or angular
base; tending to coalescence and the formation of areas with a rough
ened or scaly surface.
Symptoms.—The disease, first clearly described by Wilson,1 is
in the larger number of cases somewhat limited, but it may be more
or less widely distributed over the entire surface. The favorite sites
in the former are about the flexor aspects of the wrists and forearms
and the lower part of the leg. The limited form of the disease usually
begins insidiously. The lesions at first are discrete, scattered, bright
or dark red in appearance, slightly elevated, with a flattened, shining,
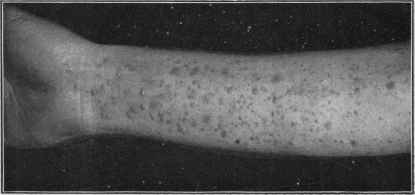
Fig. 40.—Lichen planus of moderate development, in a woman aged twenty-five,
and of several months’ duration. Practically limited to the arms and mainly on flexor
aspects.
or glistening top, in the central part of which there is usually a minute
depression. The base may be rounded; but more frequently it is irregu
larly quadrangular or angular, usually with perpendicular sides; excep
tionally minute stellate projections are noted at the base. In size they are
generally a trifle larger than a pin-head. In larger lesions, if present, there
may be, more especially after they have existed for some time, a wider
depression centrally, resulting in a slightly ringed formation; or occasion
ally new lesions spring up contiguous to the border while the central part
flattens down and partially or completely disappears. In occasional in
stances this ring-like tendency (annular lichen planus) in several or more
of the lesions or patches may be quite pronounced. Sometimes several
lesions will arrange themselves as a straight or irregular line. Excoria
tions and scratch-marks are apt to show a development of the efflores
cences. Lesions continue to arise, in the average case, close to others, and
1 E. Wilson reported a large number of cases in Jour. Cutan. Med., London, 1869,
vol. iii. No. 10.
214
1NFLAMMATIONS
several or more coalesce, and solid patches of various sizes result; the
surface of these is noted to be rough or slightly scaly. The scaliness
is generally insignificant or branny, usually quite adherent, but rarely
marked. The lesions and areas are now, as a rule, noted to be of a pur
plish color which is quite charac
teristic. Some may disappear,
leaving considerable pigmenta
tion, which is slow in fading.
In exceptional instances slight
atrophy may occur in places.1
Although some of the lesions and
areas may tend to disappear,
the eruption is, as a rule, persist
ent, new efflorescences appear
ing from time to time. The dis
ease may thus remain upon the
affected region, more particularly
the lower legs, and continue in
definitely, with but slight varia
tion.
While the plane or flat lesion
is the characteristic one of lichen
planus, in some cases there is an
admixture of a distinctly follicu-
lar and acuminate papule with or
without a slightly protruding
horny plug; exceptionally this
latter type may be predominant,
and in still rarer instances prac
tically all lesions may be of this
type.
In the leg region, and occa
sionally elsewhere—more especi
ally the forearms—the lesions
are sometimes much larger.
They are from a small to a
large pea in size, with rounded
or lenticular base, and flattened
or slightly conic in shape, dark red, brownish, or purplish in color,
with flattening of the summit or of the entire lesion; the surface
somewhat rough and branny or smooth (lichen obtusus; lichen planus
hypertrophicus). Occasionally the confluent plaques, especially about
or near the ankle, are markedly thickened, sometimes quite dark in
color, hard, rough, and wart-like—lichen planus verrucosus. Excep
tionally the lesions may be waxy in appearance. They may coalesce
1 See interesting paper on the variant forms, etc., by Crocker (“Lichen Planus: Its
Variations, Relations, and Limitations”), with discussion, Brit. Jour. Derm., 1900, p.
421; also Engman's report, “Annular Lichen Planus,” Jour. Cutan. Dis., May, 1901;
Lieberthal, “Lichen Planus Hypertrophicus.” Jour. Amer. Med. Assoc, Jan. 11, 1902.

Fig. 41.—Lichen planus—hypertrophic
papules.
LICHEN PLANUS
215
and form large areas, as with the smaller papules; the central part
of the patches may persist, or it may disappear and show staining and,
exceptionally, atrophy. In rare instances this tendency to atrophy
in lichen planus (lichen planus atrophicus1) lesions is quite striking:
the individual papules tend to enlarge peripherally to the size of a pea
or dime, thinning centrally as they enlarge, and thus presenting a ring
appearance; eventually the whole lesion may become thinned down,
disappearing, and leaving behind an atrophic white spot. Doubtless a
few of the cases of so-called white spot disease (q. v.)2 may thus originate.
In occasional instances the white spot is somewhat sclerotic and mor-
phea-like (lichen planus morphœicus (Stowers), lichen planus keloidi-
formis (Pasolow)).
The more or less generalized form of lichen planus may begin as
such or develop from the limited form.3 The lesions usually appear more
or less rapidly, are at first rather pale red than deep red; some are waxy
and semitranslucent, and conic and rounded in shape, and may or may
not have the central depression. Many, and sometimes all, the lesions are,
however, similar to those described in the limited form—angular, flat,
dark red, and umbilicated. They are apt to appear, first, or most numer
ously, on the trunk, but the extremities are also invaded, and sometimes
markedly. Sooner or later the color becomes dark red or violaceous.
There is the same tendency toward close aggregation and coalescence
here and there, with the resulting solid patch, a trifle rough and scaly.
Exceptionally in some regions the lesions appear close together, forming
narrow, bead-like bands (so-called lichen ruber moniliformis). This
formation is likewise seen in the limited form, and may constitute the
major part of the eruption, as in cases reported by Kaposi, Dubreuilh,
and G. H. Fox.
The deep-red or violaceous color of the papules of lichen planus
as ordinarily met with is usually most marked on the lower parts of
the legs. Single isolated papules are usually free from any attempt
at scaliness; exceptionally, however, a minute, thin, filmy scale sur
mounts it. Minute whitish or grayish points and striæ, and sometimes
1 Dubreuilh and Petges, “Lichen plan atrophique,” Annales, 1907, p. 715, report a
case, and review reported cases (with references). Ormsby, Lichen planus sclerosus
et atrophicus (Hallopeau); a report of six cases (five new) with a review of the litera
ture, Jour. Amer. Med. Assoc, Sept. 10, 1910, p. 901, with references and illustrations;
the writer found sites of predilection: upper portions of the trunk, about the breasts,
over the clavicles, extending over the shoulders and downward over the upper part of
the back, also the neck, axillæ, and forearms. The characteristic lesion is an irregular,
often polygonal, flat topped, white papule, with occasionally a yellowish tinge; on a
skin level or slightly elevated, with one to several or more black or dark horny, comedo-
like plugs, or minute pit-like depressions showing the sites of former plugs; isolated
and in plaques, they leave white delicate smooth scars. Radiotherapy is beneficial.
2 F. H. Montgomery and Ormsby, “White Spot Disease,” Jour. Cutan. Dis., 1907,
p. 12 (third case—lichen planus atrophicus).
3 Exceptionally such a case develops in such a way as to suggest a systemic malady.
D. W. Montgomery and Alderson report (Jour. Amer. Med. Assoc., 1909, vol. liii, p.
1457, with brief review and references) a case of lichen planus appearing acutely, the
eruption being profuse and more or less general, with brighter colored lesions, quite
fiery in appearance, with febrile and other constitutional disturbances—indicative of a
constitutional disorder—suggestively similar to the acute exanthemata. Engman and
Mook, Interstate Med. Jour., June, 1909, cite cases and circumstances favoring the
idea that this disease is a systemic one (review and references).
2l6
INFLAMMATIONS
minute red points, are not infrequently to be seen on the surface of the
lesions, more particularly those of larger size, and especially where co
alescence has taken place, the presence of which Wickham1 considers
pathognomonic of this disease. On the other hand, the shining or glazed
appearance which may be readily seen when the lesions are looked at
askant, is usually observable on all discrete lesions.
While the eruption may be quite extensive and be distributed in
smaller and larger plaques over the entire surface, it is never univer
sal. Even in extreme cases there are always some, and usually many,
free areas. It is, as a rule, more or less symmetric, although cases are
met with in which the areas of disease may be on one side, and a few in
stances are on record in which it had a zoster-like distribution. The
face is an uncommon site, even when the eruption is abundant. The
palms and soles are only occasionally involved.
Occasionally summit vesiculation is noticed in some of the lesions;
and exceptionally distinct vesicles and blebs, as in cases recorded by Unna,2
Kaposi,3 Lèredde,4 Mackenzie,5 Hallopeau and Le Sourd,6 Colcott Fox,7
Allen,8 Whitfield,9 Engman,10 and others; in rare instances it may be quite
a pronounced feature. It has been suggested that, in some of the cases
at least, the vesicular and bullous lesions might be due to the arsenic so
commonly administered in this disease, but in Whitfield‘s review of 17
collected cases, in 9 of the patients this drug had not been taken.
The mucous membrane of the mouth is quite frequently the seat of
lesions (E. Wilson, Hutchinson, Crocker, and others), and sometimes
it begins there primarily, as Thibiérge,11 Crocker,12 Petersen,13 and others
have shown; it sometimes precedes the skin eruption by some weeks, and,
in rare instances, continues practically limited to this region.14 In this
1 Wickham, Annales, 1895, p. 517.
2 Unna, Medical Bulletin, Phila., 1885, p. 145.
3 Kaposi, Archiv, 1892, pp. 340, 342, and 344.
4Lerèdde, Annales, 1895, p. 637.
5 Mackenzie, Brit. Jour. Derm., 1899, p. 26.
6 Hallopeau and Le Sourd, Jour. mal. cutan., Nov., 1899 (vesicles—in palms).
7 Colcott Fox, Brit. Jour. Derm., 1895, p. 22.
8 Allen, Trans. Amer. Derm. Assoc. for 1901; Jour. Cutan. Dis., 1902, p. 260.
9 Whitfield, Brit. Jour. Derm., 1902, p. 161 (with case and histologic illustrations).
10 Engman, Jour. Cutan. Dis., 1904, p. 207 (with case and histologic illustrations and
bibliography); Miller, “A Case of Lichen Planus Bullosus,” Jour. Cutan. Dis., 1911, p.
332 (with pertinent bibliography).
11 Thibiérge, “Des lésions de la muquese linguale dans le lichen planus,” Annales,
1885, p. 65 (this contains a review of published cases).
12 Crocker, “On Affections of the Mucous Membranes in Lichen Ruber vel Planus,”
Monalshefte, 1882, vol. i, p. 161.
13 Petersen, St. Petersburg med. Wochenschr., 1899, p. 33 (brief case report). See
also Teuton‘s paper, “Casuistisches zum Lichen ruber planus der Haut und Schleim-
haut,” Berlin, klin. Wochenschr., 1886, p. 374 (with references).
14 Some recent contributions on lichen planus of the mucous membranes are: Mew-
born, Jour. Cutan. Dis., 1905, p. 176 (case presentation). Among 10 unusual cases
reported by Beltmann (Archiv, vol. lxxv, p. 379) is one in which the only regions in
volved were the mouth and urethra; Vorner, Dermatolog. Zeitschr., 1906, vol. xiii, p. 107,
notes that umbilication may also be observed in these mucous membrane lesions;
Dubrenilk (“Histologie du lichen plan des muquenses,” Annales, 1906, p. 123) states
that the lesions of the mucous membranes are histologically essentially the same as those
of the skin); Lieberthal, “Lichen planus of the oral mucosa,” Jour. Amer. Med. Assoc,
Feb. 16, 1907 (2 cases, with illustrations); Favera, Monatshefte, 1909, vol. xlviii, p. 293
(with 2 histologic cuts and partial bibliography).
LICHEN PLANUS
217
region the disease consists of white or whitish dots or papules, plaques,
or streaks, as a rule but slightly raised. It bears a strong resemblance
to the appearances produced by cauterization with silver nitrate. As
a rule, these lesions give rise to no discomfort; occasionally there is a
feeling of slight soreness.
The glans penis has likewise been noted to be the seat of lesions, and
sometimes before their appearance elsewhere, as recorded by Bulkley1
and others.2 The eruption has also been observed on the inside and
outside of the vulva, as well as on the anal mucosa. On the glans penis
as well as on the vulva the lesions, which sometimes tend to the annular
development, are either white, when the part is habitually covered, or
of the usual color observed elsewhere when uncovered. It is thought
not improbable that in the more or less generalized cases of lichen planus,
especially the acute rapidly spreading variety, the mucous membranes of
the gastrointestinal tract may be also involved.
The disease in children usually presents the same symptoms as
when occurring in adults, but there is a type occurring in infants, de
scribed by Crocker3 and Colcott Fox,4 in which the eruption (quoting
Crocker) comes out acutely in groups, each papule of which is some
times acuminate at first, but the top seems to die down and a scale
comes off, leaving a smooth, shining, angular papule, of a brighter red
than usual, though it may get a purplish tint subsequently. Limbs,
trunk, or both may be the seat of the eruption. There is considerable
itching.
The course of lichen planus is in most cases slow, insidious, and
chronic. In some instances, it is true, as already remarked, the out
break may be extensive and somewhat rapid, but, as a rule, the erup
tion is slow in development, and in the majority of patients somewhat
limited in extent. In many of the limited cases, after reaching a cer
tain point, it may remain practically stationary for a long time, or
there is retrogression of some lesions along with the appearance of
new papules. Exceptionally, it tends after a time to disappear spon
taneously, but, as a rule, it is persistent. There are rarely any gen
eral symptoms except in cases of acute outbreaks or exacerbations,
and even then but slight and transitory. In more or less generalized
cases a marasmic tendency has occasionally been recorded.
The subjective symptoms, consisting of burning and itching, but
usually the latter, vary somewhat in different cases and often in the
same case. Occasionally the itching is not troublesome or so slight
as to give rise to no complaint; generally, however, it is an annoying
symptom, and sometimes so intense as to deprive the patient of restful
sleep.
Etiology.—The disease is not frequent. It is seen in both sexes,
and most commonly during active adult life, being rare in children.
1 Bulkley, Arch. Derm., 1881, p. 135.
2 Fordyce, Jour. Cutan. Dis., 1912, p. 351, demonstrated a case with lesions on
the penis and mucous membrane of inner side of cheek—nowhere else.
3 Crocker, Diseases of the Skin, first ed., 1888, p. 215; second ed., 1893, p. 302.
4 Cotcott Fox, “Notes on Lichen Planus in Infants,’’ Brit. Jour. Derm., 1891, p.
201 (7 cases).
2l8
INFLAMMATIONS
Exceptionally the malady has been observed in two or three members
of the same family (Brocq, Lustgarten, Ormerod, Ledermann, Jadassohn,
Hallopeau, F. Veiel, and others).1 It is most frequently observed in
those of the neurotic class, after prolonged worry, overwork, anxiety,
nervous shock, or exhaustion; and is met with relatively oftener in private
than dispensary practice. In fact it would seem, in most cases at least,
that the disease is the result of disturbance of the nervous system. This
appears to have further support in the fact that it has occasionally been
noted to follow nerve distribution and also nerve injuries. It, however,
occurs in those apparently well nourished as well as in those showing
malnutrition.
Almost all authors of note recognize its frequency among the ner
vously depressed and exhausted. Duhring2 holds strongly to this view,
stating that, according to his experience, patients are generally found to
be suffering from debility arising from improper nourishment, overwork,
nervous depression, and similar conditions, and that nervous symp
toms are often prominent. I have myself long had under observation 2
cases (women) who have had recurrences when worn out with prolonged
winter social exactions. A few others hold the view of a possible systemic
infection.3
According to Crocker and Colcott Fox, the infantile cases seem, for
the most part, to occur in those whose vitality has been weakened by
constitutional taint, such as scrofula, syphilis, and the like.
Pathology.—Lichen planus is apparently an inflammatory proc
ess, but what the initial exciting pathologic factor is remains as yet
unknown. That it is a neuropathic affection seems probable, Col-
cott Fox suggesting that the first step may be a neuroparalytic hyper-
emia. The question 4 of its relationship to pityriasis rubra pilaris (lichen
ruber) is still an unclosed one, although the large preponderance of
opinion considers them two distinct affections. It seems certain, how
ever, that in some cases of extensive lichen planus occasionally papules
similar or closely similar to those characterizing pityriasis rubra pilaris
(lichen ruber) are observed.5
The pathologic anatomy has been studied by Robinson, Crocker,
Török, Unna, Polano, Fordyce, Sabouraud, and others. The disease
1 F. Veiel, “Lichen ruber planus als Familienerkrankung,” Archiv, vol. xciii, H. 3,
1908.
2 Duhring, Diseases of the Skin, third ed., 1882, p. 259; Spiethoff reports (Archiv,
Jan., 1911, Bd. cv, H. 1 and 2, p. 69) a case in which there was an associated pernicious
anemia.
3 Norman Walker (Introduction to Dermatology) thinks it possible that it may
later be found among the infective granulomata.
4 See Discussion, Compt. Rend., “Congréss Internat. de Derm, et de Syph.,” Paris,
1889.
5 Kaposi believes that lichen planus, sometimes called the lichen planus of Wilson,
is related to the malady described by Hebra as lichen ruber, and to the former he gave
the name lichen ruber planus, and to the latter, lichen ruber acuminatus. This view
obtained for some years, but was followed by a more or less general reversion, and
the acceptance of the opinion that these two so-called types or forms really represented
two distinct and separate cutaneous maladies, although a few eminent diagnosticians, as
Neumann and Hebra, Jr., as well as several others, have noted cases in which the two
coexist. Lichen ruber acuminatus, Kaposi further considers, as is now generally ad
mitted, as identical with pityriasis rubra pilaris.
LICHEN PLANUS
219
has its seat in the upper part of the corium, and usually around a sweat-
duct. The hair-follicles have no determining influence in the situa
tion of the papules. The changes are somewhat different, depending
upon the duration and character of the lesion. The rete and corneous
layer are noted to be thickened, and the papillæ enlarged, the vessels
of the latter showing dilatation. Fordyce1 noted the earliest changes
to consist in dilatation of the vessels and lymph spaces of the papillæ.
The papule results (Sabouraud)2 from a proliferation of the mononuclear
cells in the papillæ crowding out the interpapillary processes of the
epidermis, becoming edematous to a variable degree, even in some in
stances, to the degree of vesiculation. The central point of the depression
usually corresponds to the sweat-duct orifice, the depression resulting
from reabsorption and degeneration of the infiltration; the sweat-glands
are not affected.
The first characteristic change noted in the epidermis is thought to
be an acanthosis, followed by epithelial atrophy, and a hyperkeratosis,
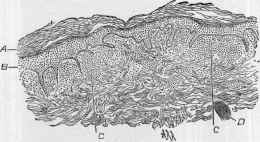
Fig. 42.—Lichen planus—section of two contiguous papules of not very long stand
ing (low magnification): A, Corneous layer, thickened slightly; B, rete and granular
layers, considerably thickened; C, C, round-cell collection in upper part of the corium
and papillæ, some of the latter thus crowded out, others enlarged by the increase in
length of the interpapillary rete; D, muscle bundle (courtesy of Dr. A. R. Robinson).
intercellular edema, and colloid degeneration of the prickle-cells. Histo-
logically, the mucous membrane lesions present the same features as those
of the skin.
Diagnosis.—The irregular and angular outline, the flattened top,
the slight central depression, the glistening or glazed appearance, the
dull red or purplish color, the tendency to patch-formation of a slightly
rough and scaly surface, with outlying typical papules, together with the
history and course and usually itchy character—are features which are
peculiar to this disease, and will generally prevent an errror in diagnosis.
The larger patches look somewhat like psoriasis, but the distribution is
different and they are less scaly, of different color, and about the edges
are to be found the characteristic papules. A patch of psoriasis is due to
peripheral extension, that of lichen planus usually to accretion of new
papules.
1 Fordyce, “The Lichen Group of Skin Diseases; A Histologic Study,” Jour. Cutan.
Dis., 1910, p. 57 (with excellent histologic illustrations).
2 Sabouraud, Annales, 1910, p. 491 (pathologic anatomy; excellent illustrations).
220
INFLAMMATIONS
While the patches of the disease may resemble squamous eczema,
the characters of the papules, always to be found, are essentially dif
ferent; and in an extensive papular or scaly eczema there is often the
presence of a few intermingled vesicles or a history of such or of oozing;
lichen planus is in almost all cases a dry disease throughout, and the
lesions are papular and not vesicular, moreover, the papules of eczema
are rounded or acuminate. It is only in exceptional instances that some
of the lesions of lichen planus may show vesicular and bullous develop-
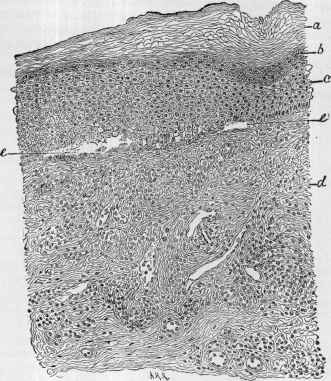
Fig. 43.—Lichen planus—section from a chronic patch (moderately high magnifica
tion) : a, b, c, Show respectively the corneous layer, granular, and rete—all consider
ably thickened; e, e, microscopic cavities, with serous exudate; d, corium, infiltrated
with exuded round cells, and with marked increase in the size of the connective-tissue
corpuscles (courtesy of Dr. A. R. Robinson).
ment—all of the other papules preserving their usual characteristics
throughout.
I have known it to be mistaken for the miliary papular syphiloderm,
but in this latter the lesions are usually rounded or conic, and, while
tending to aggregate, do not form solid areas, are of a somewhat different
color, and almost invariable show some scattered miliary pustules, and
often a few larger pustules; moreover, it being an eruption of the active
stage of syphilis, there are corroborative signs of that disease to be
found.
LICHEN PLANUS
221
From pityriasis rubra pilaris the following differences are usually
given: the lesions of pityriasis rubra pilaris are round or conic, not shining
or glistening, not irregular in outline; are rarely umbilicated; show
a scaly film on the summit; are red, and never violaceous, in color;
and while the eruption is limited at first, it tends to general involve
ment. According to Hebra's own description, however, there would
seem at times a clinical resemblance in some of the papules of the two
affections. Those of pityriasis rubra pilaris are, however, seated about
the hair-follicles.
Prognosis.—Its natural course is persistent and often progressive,
and shows little tendency to spontaneous recovery. With treatment
it can be cured, sometimes in a few months, but oftener a much longer
time is required. There is in some cases a disposition to one or more
recurrences. The pigmentation finally disappears, but sometimes
months elapse before it is entirely gone; occasionally on the legs the
discoloration is permanent.
Treatment.—The patient is to have the benefit of good plain
food, hygienic living, and, when possible, outdoor life and freedom
from mental worry or care. The various tonics and cod-liver oil may
be prescribed when indicated. The main remedies in this disease,
however, are arsenic, mercury, quinin, and strychnin. Arsenic in many
cases has a direct specific influence, given in increasing doses to the
point of tolerance, and continued for some time; mercury is also valuable
and seems to have a direct action in some instances. These two drugs,
and especially the former, are, if no contraindications exist, to be, as a
rule, always prescribed, and, along with other indicated remedies, usually
lead to recovery. The former is given in the beginning dosage, three
times daily, of 2½ or 3 minims (0.165 or 0.2) of Fowler's solution or sodium
arsenate solution, or the equivalent of arsenious acid, and gradually in
creased to 5, 6 (0.33, 0.4), or more; larger doses than 10 minims (0.65)
are rarely required, and if no benefit is obtained with this amount, it is not
likely to ensue from a greater quantity. Mercury can be given in the
form of the corrosive chlorid (Norman Walker), or the biniodid in the
dose of 1/32 to 1/12 grain (0.002 to 0.0055), or as the protiodid in dosage of 1/8
to ½ grain (0.008 to 0.033). Quinin is also valuable, and should be given
in fairly full doses—9 to 15 grains (o.6 to 1.) daily. Hartzell has had
favorable action in some instances from sodium salicylate.1 Strych
nin is an excellent tonic in these cases. Constitutional treatment2
should, as a rule, be continued, in somewhat lessened dosage, one or two
months after the eruption has disappeared.
External treatment is of great importance, both for influencing
the eruption and for allaying the itching usually present, and in the
limited form of the disease often alone suffices to bring about a cure.
1 Hartzell, “The Salicylates in the Treatment of Lichen Planus,” Jour. Amer. Med.
Assoc, 1907, vol. xlix, p. 225 (with a report of some unusual forms).
2Hutchins, Jour. Cutan. Dis., 1912, p. 615, describes an interesting case of dif
fused lichen planus (in a male, six years of age), followed by vesicobullous infected
lesions, some of the vesicles and bullæ where lichen planus lesions had not been; cured
by an autogenous vaccine made from culture of the staphylococcus obtained from a
vesicle.
222
INFLAMMATIONS
In cases of any considerable extent alkaline baths every other day, or
in irritable cases, bran, gelatin, or starch baths daily, are of service, to
be followed on the patches with ointment applications or with lotions.
The most efficient application in the general run of cases is liquor car-
bonis detergens; this is to be applied at first diluted with 10 to 15 parts
water, but if no irritation is produced, it may gradually be strengthened,
and in some cases can be used pure. It is to be dabbed on thoroughly
twice daily, and oftener if the itching demands it. It the skin becomes
unpleasantly dry or harsh, its application can occasionally be followed
with cold cream; or it may be prescribed in ointment form, 1 or 2 drams
(4. to 8.) to an ounce (32.) of simple cerate or a mixture of simple cerate
and cold cream. The vegetable tars, expecially the oil of cade and oil of
birch (oleum rusci), are also excellent in chronic cases, but are stronger
than liquor carbonis detergens, and have a more marked and persistent
odor; they are best applied in ointment form, 1 to 2 drams (4. to 8.) to the
ounce (32.). In acute inflammatory and irritable cases the calamin-zinc-
oxid lotion and the plain or carbolized boric acid lotion act satisfactorily,
stronger applications—liquor carbonis detergens—being resorted to
later. This calamin-and-zinc-oxid lotion and the other mild lotions used
in eczema can also be advised for the disease occurring in infants and
children. For thick, hardened, or verrucous areas, a 10 to 20 per cent,
salicylic acid rubber plaster or plaster-mull can be used until the thick
ness is reduced; or paintings with varying strength of caustic potash solu
tions, beginning with the liquor potassæ, can be used cautiously, washing
off immediately afterward, and supplementing with a mild ointment, such
as zinc-oxid or diachylon ointment. In obstinate patches of this charac
ter stimulation or slight superficial cauterizing action with carbon-dioxid
snow (q. v.) can be cautiously tried.
When the lesions are close together and patchy, as on the fore
arms, the galvanic current, of 4 to 10 milliampères in strength, applied
three or four times weekly, has had in some of my cases a material
influence; the application should be rapidly labile, except over thick
ened areas, where the electrodes can be held stationary for one or two
minutes. In these cases, too, the static current applied with the roller
electrode and the high-frequency current applied with the flat vacuum
electrode are also sometimes of service.
A Chronic Itching Lichenoid Eruption of the Axillary and Pubic
Regions.—Brocq, Fox, Fordyce, Haase,1 and others have reported
cases, few in number, characterized by a more or less limited and
localized patch formation usually in the axillary and pubic regions,
made up of closely set, more or less coalescent, somewhat firm or hard
pin-head to pea-sized papules, seemingly seated on, and an intimate
1 G. H. Fox, “Two Cases of a Rare Papular Disease Affecting the Axillary Regions,”
with histopathologic report by Fordyce, Jour. Cutan. Dis., 1902, p. 1 (with histologic
cuts); Fordyce, “A Chronic Itching, Papular Eruption of the Axillae and Pubes; Its
Relation to Neurodermatitis,” Trans. Amer. Derm. Assoc., for 1908, p. 118 (with case
and histologic cuts); Haase, “A Chronic, Itching Papular Eruption of the Axillae,
Pubes, and Breast,” Jour. Amer. Med. Assoc, Jan. 21, 1911 (with case and histologic
cuts).
LICHEN PLANUS
223
part of, a locally infiltrated thickened skin. Some of the lesions show
a slight central depression, some are flattened, some rounded, and
most of them showing a central grayish plug. The lines of the skin
of the involved area are accentuated, and when the skin is put on
the stretch markedly so. The lesions and patch are of normal skin
color or dirty gray, sometimes with a dull violet or pinkish tinge.
The process is, as a rule, insidious in its appearance and is an ex
tremely sluggish one, very slow in progress and after a time usually
remaining stationary. The itching is often a prominent symptom, occa
sionally at times almost intolerable, and some of the papules are generally
noted to be excoriated. The itching is often the first symptom observed,
leading to rubbing and scratching, and being sooner or later followed by
the papulation and thickening. The hairy parts of the axillary and pubic
regions are favorite sites—less frequently about the nipples also. The
hairs of the affected part, after the appearance of the lesions, usually
become brittle and lusterless, and to an extent, or even completely,
break off or fall out. The malady is persistent and rebellious to treatment.
The clinical picture is suggestive of the combined symptomatology of a
pityriasis rubra pilaris, lichen planus, and a papular selerous eczema. It
represents a condition or class of cases called “lichenification” by the
French; and Fordyce and Haase believe it should be placed under Brocq's
group of “chronic circumscribed neurodermatitis (névrodermite chronique
circonscrite).“ Most observers have doubtless placed these rather rare
cases as variant examples of lichen planus or eczema. Histologically
there were found acanthosis and some parakeratosis, with hypertrophied
papillæ, edematous at their tips; lymphocytic infiltration about the ves
sels and pilosebaceous apparatus, with, in some instances, involvement of
the sweat-gland apparatus also.
Lichen nitidus is a rare eruption, first described by Pinkus
(1901), and since by this same writer (9 cases in all), Lewandowsky
(2 cases), Arndt (12 cases),1 Kyrle and McDonagh (1 case),2 and Sutton.3
The lesions are small, usually flat, sharply margined papules, roughly
circular or polygonal in shape, scarcely raised above the level of the
skin, of skin color, pale red, or yellowish brown. They are almost
uniformly of the same size, and often a minute aperture can be detected
in the center of the papule. The lesions are usually disseminated,
never coalesce or show any disposition to form groups, although some
times they may tend to pack together closely. They are persistent
and without change; after years they may spontaneously disappear,
leaving no trace. The favorite regions are: the genital organs (its most
typical site), abdomen, especially about the umbilicus, the flexures of
1 Arndt, Dermatolog. Zeitschr., 1909, vol. xvi, H. 9 and 10 (clinical, histologic, with
review); good abstract in Brit. Jour. Derm., Jan., 1910.
2 Kyrle and McDonagh, Brit. Jour. Derm., 1909, p. 339 (case, a girl aged eighteen;
eruption more or less generalized; histologic plate; and résumé of Pinkus’ cases).
3 Sutton, Jour. Cutan. Dis., 1910, p. 597, case, male, aged thirty-five; eruption on
anterior fold of both axillae, in groin, around the umbilicus, upper anterior surface of
each forearm, flexor surfaces of the wrists, and dorsal aspect of both thumbs; ex
perimental inoculations (two guinea-pigs) negative; histologic and case illustrations
with review and references.
224 INFLAMMATIONS
the elbows, and the palms. There are no subjective symptoms, and this
and the fact that the eruption is insignificant, usually on covered parts,
and often scarcely noticeable except upon close examination, probably
explain why so far all the cases have only come accidentally under obser
vation; with one exception they were all male subjects. Nothing is
known as to its etiology and pathogenesis, although Kyrle and McDonagh
believe it is probably brought about by a tuberculous toxin. Histolog-
ically, a lesion has a structure resembling tubercle.
The papules have some resemblance to those of lichen planus, and
also a variable suggestiveness of small multiple flat warts, the flat form
of lichen scrofulosum, and lichenoid syphiloderm. The malady does
not seem to be materially influenced by treatment.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |